

Volume 11, Issue 4 (2025)
Pharm Biomed Res 2025, 11(4): 331-338 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salehifar E, Bagherzadegan Z, Ala S, Ramezaninejad S. Albumin Utilization Evaluation in a Teaching University Hospital in Iran. Pharm Biomed Res 2025; 11 (4) :331-338
URL: http://pbr.mazums.ac.ir/article-1-711-en.html
URL: http://pbr.mazums.ac.ir/article-1-711-en.html



1- Department of Clinical Pharmacy, Pharmaceutical Sciences Research Center, Faculty of Pharmacy, Institute of Herbal Medicines and Metabolic Disorders, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Pharmaceutical Care, Emam Khomeini Hospital, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Clinical Pharmacy, School of Pharmacy, Babol University of Medical Sciences, Babol, Iran.
2- Department of Pharmaceutical Care, Emam Khomeini Hospital, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Clinical Pharmacy, School of Pharmacy, Babol University of Medical Sciences, Babol, Iran.
Full-Text [PDF 682 kb]
(189 Downloads)
| Abstract (HTML) (469 Views)
Full-Text: (91 Views)
Introduction
Drug utilization evaluation (DUE) studies assess the appropriateness of a particular prescribed drug indication, the drug’s dosage, the length of treatment, and drug-related monitoring [1]. The clinical needs of patients and reliable guidelines should be the basis for prescribing medications [2]. Recently, DUE studies have gained popularity as a useful technique for determining if drug use is appropriate in the course of treatment [3].
The World Health Organization (WHO) defines drug utilization as the marketing, distribution, prescription, and use of drugs in society, considering medical, social, and economic consequences [4]. DUE research holds particular importance for expensive drugs and those with a narrow therapeutic index, given their larger clinical impact and financial burden on healthcare systems [5].
Albumin is the most abundant protein in the blood and makes up approximately 50% of all plasma proteins. It is synthesized by the liver, secreted immediately without storage, and is physiologically regulated by nutritional status and colloid osmotic pressure. Normal blood plasma concentrations range from 3.5 to 5 g, and 60% of total albumin is found in the interstitial space [6].
Human albumin solution (HAS) is a colloidal preparation with a high cost and is commonly used clinically. HAS comes in 5%, 20%, and 25% formulations, each with unique physiologic properties that should not be used interchangeably. The applications of 5% solutions with osmotic pressure equal to that of normal plasma differ significantly from those of the hyperosmotic 20% and 25% solutions [7]. It is essential to establish a workable protocol for using albumin products and limit their use due to their high cost, the rise in inappropriate use, the difficulty of their production, the risk of disease transmission, and the availability of other affordable alternatives with the same effectiveness [7]. Misuse of albumin places an excessive financial burden on health systems and is a significant pharmacoeconomic issue, especially during periodic shortages in Iran and globally, alongside limited supply resources [8, 9].
Albumin, as a colloid solution, offers greater benefits than non-protein colloids in both efficacy and safety [7-11]. Nonetheless, albumin is misused in several clinical conditions: Pancreatitis, ascites that responds to diuretic therapy, nephrotic syndrome that is not linked to hypovolemia and or pulmonary edema, and the treatment of malnutrition in critically ill patients [1, 7, 12]. Several studies have reported albumin misuse in the literature, showing its negative clinical and economic impacts [9, 10, 11, 13, 14]. According to a study conducted in Brazil, about 55.1% of cases were inappropriate for albumin request [14]. This misuse could be attributed to the absence of collective protocols defining appropriate albumin indications to guide healthcare providers, as well as the lack of restrictive strategies for prescribing and dispensing albumin [15]. Following clinical guidelines minimizes inappropriate albumin use. Clinical pharmacists and PharmDs play a critical role in improving albumin usage, optimizing medication management, enhancing patient outcomes, and reducing unnecessary drug use or hospital stays [16, 17]. A small number of studies examined the effects of clinical pharmacist interventions on albumin use in intensive care units (ICUs) and found that these interventions resulted in both favorable clinical and financial outcomes [11, 15]. This study aimed to assess albumin use and evaluate compliance with FDA-approved guidelines in hospitalized patients.
Materials and Methods
This research was a retrospective study of patients receiving albumin at Imam Khomeini Educational Hospital, affiliated with Mazandaran University of Medical Sciences, Sari City, Iran. The recruitment period was from March 20, 2023, to March 19, 2024. Data were collected from the albumin request form completed by various departments and sent to the Pharmaceutical Care Department.
The reason for choosing this time was that the hospital mainly supplied albumin and had no significant restrictions on its supply, so patients did not need to visit pharmacies outside the hospital to obtain it.
We gathered information on albumin utilization using a standardized albumin prescribing form, developed by the Iranian Food and Drug Organization and based on validated references [18, 19], and made it available to hospitals to promote rational albumin prescribing.
Since there is no comprehensive international guideline available regarding the rational indications of albumin usage, the appropriateness of albumin prescription was evaluated using the latest evidence‑based studies and guidelines [7-12]. The appropriate and inappropriate indications are shown in Table 1.
.PNG)
.PNG)
The quantitative variables examined in this study were age, weight, initial albumin level, total protein level, prescribed albumin dose, and duration of albumin administration. The qualitative variables examined included gender, hospitalization department, and indication for albumin administration. Blood serum albumin levels were measured before administering albumin and rechecked 72 hours after the first dose.
Data were transferred to SPSS software, version 20 for statistical analysis. The Shapiro-Wilk test was used to assess the data distribution. The descriptive assessment was reported as Mean±SD for numerical variables and as median for numerical variables; numbers and percentages were reported for nominal variables.
Results
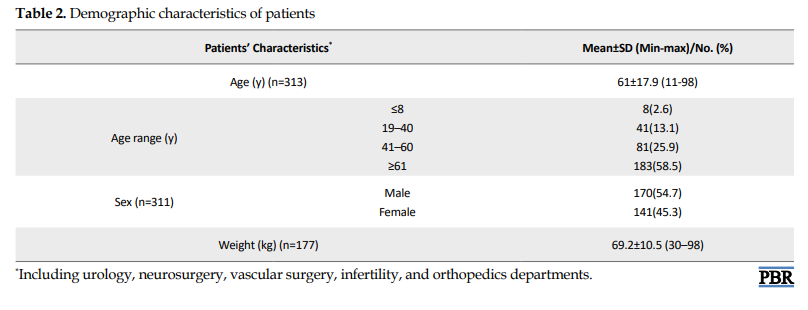
Demographic features of patients were presented in Table 2. Of the 313 included patients, 55% were male. The patient age range was 11 to 98 years, with an average age of 61 years. Approximately 60% of the patients were older than 60 years.
The departments that prescribed albumin the most were ICUs (43%, total of 4 departments); hematology, oncology, and oncosurgery (26.9%); and internal medicine departments (16.4%) (Figure 1).
.PNG)
Table 3 presents the indications for albumin administration based on the items mentioned in the albumin request form. Albumin level less than 2.5 g/dL for 3 days (25.4%), ascites or generalized edema (24.4%), and hepatorenal syndrome (HRS) (13%) were the most common reasons for albumin administration. In 7 cases (2.3%), albumin administration was not based on any of the official indications mentioned in the form.
.PNG)
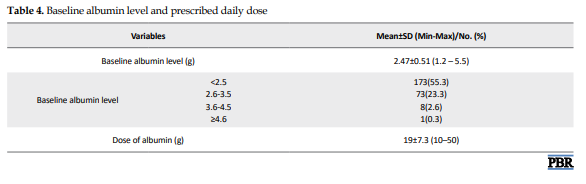
The patients’ minimum albumin level at the start of albumin therapy was 1.2 g/dL, and the maximum was 5.5 g/dL. The daily dose of 20% albumin solution (10 g) was a minimum of 1 vial (50 mL) and a maximum of 5 vials (250 mL), with an average of 19 g daily (approximately 2 vials) (Table 4). In 82 patients (32.1%), serum albumin levels were greater than 2.5 g/dL at the time of albumin administration, of whom 46(56%) were above the recommended cut-off for the indication.
According to the protocol defined by the Iranian Food and Drug Administration (FDA Iran), the duration of albumin treatment should be stated on the albumin request form. In this study, only 1 patient (0.3%) had the duration of albumin treatment stated.
Another item on the albumin request form is the measurement of serum albumin levels 72 hours after starting albumin, which was not recorded for any of the 313 patients.
Discussion
The WHO uses a variety of intervention techniques, such as administrative, training, and monitoring measures, to encourage the prudent use of medications and enhance drug management programs. It is acknowledged that these strategies make medications more readily accessible within public health organizations, thereby helping low-income patients financially [8].
If medications are prescribed and used appropriately, more patients could be served and supported while keeping the limited medical budget in mind. As a result, it is critical to identify the costly but often prescribed drug productions and establish appropriate consumption patterns. DUE is a time-consuming process, but it has been effective in starting a discussion between physicians and pharmacists to achieve high standards for drug use in hospitals. It aids in revealing the drug administration patterns in the institutions under investigation [9].
Despite its high cost, albumin remains a commonly used medication. According to the most recent evidence-based research and recommendations [18], we assessed the appropriateness of albumin use.
In the present study, we evaluated the administration of albumin based on rational-use protocols, which provide an evidence-based assessment of prescribing by healthcare practitioners. Our study showed that albumin was used appropriately in 292 of 313 patients (93.2%).
Improper use of albumin results in significant resource waste and increases the likelihood of undesirable effects. DUEs can be used to identify patterns of albumin use in facilities, and the results could help physicians change their practices.
Because albumin and colloidal oncotic pressure are closely related, hypoalbuminemia may lead to or be the cause of edema [20]. Furthermore, a normal albumin level maintains a balance between the hydrostatic and colloid osmotic pressures inside vessels, preventing the development of edema [18]. Consequently, it is thought that albumin, which has diuretic and water-retention properties, can be used to treat edema caused by hypoalbuminemia [21, 22]. In our study, 2.3% of patients used the medication off-label during the research period.
Hypoalbuminemia was one of the most common reasons for albumin treatment in this analysis, accounting for 76 prescriptions (25.4%). A serum albumin concentration of less than 3.5–4 g/dL is known as hypoalbuminemia, and it is linked to several different clinical disorders [19]. Hypoalbuminemia has been linked to poor outcomes in different critical conditions [12, 20]. However, several studies have shown no discernible impact of albumin administration on mortality or morbidity in hypoalbuminemic patients [7]. Reduced serum albumin concentration alone is therefore not regarded as a good enough rationale for albumin replacement in several guidelines. Finding and treating the underlying causes of the hypoalbuminemia is a helpful practice for these patients.
On the other hand, some recommendations state that albumin should be administered only when the serum albumin level is less than 2.5 g/dL [22, 23]. In this study, 76 patients with an albumin level below 2.5 were candidates for receiving albumin vials. Approximately one-third of patients had serum albumin levels above the guideline cut-off (2.5 g/dL) at the time of albumin initiation, and in 3.6% of patients, this level was above 3.5 g/dL.
As noted above, the duration of albumin treatment should be stated on the albumin request form. In this study, only 1 patient (0.3%) had the duration of albumin treatment stated.
The measurement of serum albumin levels 72 hours after starting albumin is another item on the albumin request form, but none of the 313 patients had this information documented. It is crucial to monitor patients receiving albumin for 72 hours after the start of administration to assess ongoing need. Regretfully, this study found that no patients had this evaluation done after 72 hours. Patient monitoring and re-evaluation at least 72 hours after administration can minimize irrational drug administration and the associated financial burden, as the duration of albumin administration and the need for ongoing treatment vary by indication and patient factors [24].
In contrast to other studies, the most common improper use of albumin was observed after cardiac surgery in the studies by Jahangard-Rafsanjani et al. [25] and Kazemi et al. [5] at Shariati and Shaheed Rajaei hospitals in Tehran City, Iran. In addition, as in our investigation of irrational albumin utilization at Imam Reza Hospital in Tabriz City, Iran, Shafiee et al. [26] identified hypoalbuminemia and nutritional support as the most common causes.
A small number of studies examined the role of clinical pharmacists in optimizing albumin use, though most focused on developing albumin protocols [13, 27]. In addition to developing an approved protocol, Buckley et al. noted that clinical pharmacists assessed all albumin orders for appropriateness and intervened when necessary. In their report, inappropriate albumin consumption has significantly decreased by 72.9% [15]. According to Lyu et al. and Buckley et al. using established techniques resulted in an absolute decrease in albumin misuse of 50.9% and 36%, respectively [13, 15]. According to another study conducted in critically ill patients, the clinical pharmacists’ actions greatly improved the appropriateness of albumin usage in the ICU from 16.3% in the retrospective phase to 84.1% in the implementation phase [28]. Our study showed that the presence of an albumin prescription form in wards and pharmacist supervision were able to minimize irrational albumin prescriptions, at least in terms of inappropriate indications. However, the duration and need for continued treatment were not in compliance with the guideline, and we believe that the pharmacist’s attendance in the clinical wards could help minimize these errors. Given the financial burden and the local and even global shortage of albumin, greater pharmacist supervision of albumin request forms and compliance with guidelines can improve the rational prescribing and use of albumin.
This study represents a single teaching hospital site, and further research is needed to determine if these trends are present in other community hospital settings. The limitations of this study include the lack of investigation into the duration of albumin consumption and the total grams of albumin received by each patient, which should be examined more closely in future studies.
Conclusion
Hypoalbuminemia and ascites were the most common reasons for the administration of albumin. On the other hand, our study showed that the presence of an albumin prescription form in hospital wards and the presence of a pharmacist could minimize the irrational prescription of this drug. This study showed significant deviations from the albumin prescription protocol. Some aspects of albumin prescribing, including the minimum cut-off for starting albumin, the duration of use, and rechecking the albumin level, were not adequately considered by physicians. These findings emphasize a more sophisticated focus on the albumin prescribing in an attempt to minimize the irrational prescription of this expensive and valuable drug.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and Final approval: All authors; Data collection and clinical studies: Ebrahim Salehifar, Zahra Bagherzadegan, and Shahram Ala; Data analysis and statistical analysis: Ebrahim Salehifar; Investigation and data acquisition: Sima Ramezaninejad; Writing the original draft: Sima Ramezaninejad; Review and editing: All authors; Supervision: Sima Ramezaninejad.
Conflict of interest
The authors declared no conflict of interest.
References
Drug utilization evaluation (DUE) studies assess the appropriateness of a particular prescribed drug indication, the drug’s dosage, the length of treatment, and drug-related monitoring [1]. The clinical needs of patients and reliable guidelines should be the basis for prescribing medications [2]. Recently, DUE studies have gained popularity as a useful technique for determining if drug use is appropriate in the course of treatment [3].
The World Health Organization (WHO) defines drug utilization as the marketing, distribution, prescription, and use of drugs in society, considering medical, social, and economic consequences [4]. DUE research holds particular importance for expensive drugs and those with a narrow therapeutic index, given their larger clinical impact and financial burden on healthcare systems [5].
Albumin is the most abundant protein in the blood and makes up approximately 50% of all plasma proteins. It is synthesized by the liver, secreted immediately without storage, and is physiologically regulated by nutritional status and colloid osmotic pressure. Normal blood plasma concentrations range from 3.5 to 5 g, and 60% of total albumin is found in the interstitial space [6].
Human albumin solution (HAS) is a colloidal preparation with a high cost and is commonly used clinically. HAS comes in 5%, 20%, and 25% formulations, each with unique physiologic properties that should not be used interchangeably. The applications of 5% solutions with osmotic pressure equal to that of normal plasma differ significantly from those of the hyperosmotic 20% and 25% solutions [7]. It is essential to establish a workable protocol for using albumin products and limit their use due to their high cost, the rise in inappropriate use, the difficulty of their production, the risk of disease transmission, and the availability of other affordable alternatives with the same effectiveness [7]. Misuse of albumin places an excessive financial burden on health systems and is a significant pharmacoeconomic issue, especially during periodic shortages in Iran and globally, alongside limited supply resources [8, 9].
Albumin, as a colloid solution, offers greater benefits than non-protein colloids in both efficacy and safety [7-11]. Nonetheless, albumin is misused in several clinical conditions: Pancreatitis, ascites that responds to diuretic therapy, nephrotic syndrome that is not linked to hypovolemia and or pulmonary edema, and the treatment of malnutrition in critically ill patients [1, 7, 12]. Several studies have reported albumin misuse in the literature, showing its negative clinical and economic impacts [9, 10, 11, 13, 14]. According to a study conducted in Brazil, about 55.1% of cases were inappropriate for albumin request [14]. This misuse could be attributed to the absence of collective protocols defining appropriate albumin indications to guide healthcare providers, as well as the lack of restrictive strategies for prescribing and dispensing albumin [15]. Following clinical guidelines minimizes inappropriate albumin use. Clinical pharmacists and PharmDs play a critical role in improving albumin usage, optimizing medication management, enhancing patient outcomes, and reducing unnecessary drug use or hospital stays [16, 17]. A small number of studies examined the effects of clinical pharmacist interventions on albumin use in intensive care units (ICUs) and found that these interventions resulted in both favorable clinical and financial outcomes [11, 15]. This study aimed to assess albumin use and evaluate compliance with FDA-approved guidelines in hospitalized patients.
Materials and Methods
This research was a retrospective study of patients receiving albumin at Imam Khomeini Educational Hospital, affiliated with Mazandaran University of Medical Sciences, Sari City, Iran. The recruitment period was from March 20, 2023, to March 19, 2024. Data were collected from the albumin request form completed by various departments and sent to the Pharmaceutical Care Department.
The reason for choosing this time was that the hospital mainly supplied albumin and had no significant restrictions on its supply, so patients did not need to visit pharmacies outside the hospital to obtain it.
We gathered information on albumin utilization using a standardized albumin prescribing form, developed by the Iranian Food and Drug Organization and based on validated references [18, 19], and made it available to hospitals to promote rational albumin prescribing.
Since there is no comprehensive international guideline available regarding the rational indications of albumin usage, the appropriateness of albumin prescription was evaluated using the latest evidence‑based studies and guidelines [7-12]. The appropriate and inappropriate indications are shown in Table 1.
The quantitative variables examined in this study were age, weight, initial albumin level, total protein level, prescribed albumin dose, and duration of albumin administration. The qualitative variables examined included gender, hospitalization department, and indication for albumin administration. Blood serum albumin levels were measured before administering albumin and rechecked 72 hours after the first dose.
Data were transferred to SPSS software, version 20 for statistical analysis. The Shapiro-Wilk test was used to assess the data distribution. The descriptive assessment was reported as Mean±SD for numerical variables and as median for numerical variables; numbers and percentages were reported for nominal variables.
Results
Demographic features of patients were presented in Table 2. Of the 313 included patients, 55% were male. The patient age range was 11 to 98 years, with an average age of 61 years. Approximately 60% of the patients were older than 60 years.
The departments that prescribed albumin the most were ICUs (43%, total of 4 departments); hematology, oncology, and oncosurgery (26.9%); and internal medicine departments (16.4%) (Figure 1).
Table 3 presents the indications for albumin administration based on the items mentioned in the albumin request form. Albumin level less than 2.5 g/dL for 3 days (25.4%), ascites or generalized edema (24.4%), and hepatorenal syndrome (HRS) (13%) were the most common reasons for albumin administration. In 7 cases (2.3%), albumin administration was not based on any of the official indications mentioned in the form.
The patients’ minimum albumin level at the start of albumin therapy was 1.2 g/dL, and the maximum was 5.5 g/dL. The daily dose of 20% albumin solution (10 g) was a minimum of 1 vial (50 mL) and a maximum of 5 vials (250 mL), with an average of 19 g daily (approximately 2 vials) (Table 4). In 82 patients (32.1%), serum albumin levels were greater than 2.5 g/dL at the time of albumin administration, of whom 46(56%) were above the recommended cut-off for the indication.
According to the protocol defined by the Iranian Food and Drug Administration (FDA Iran), the duration of albumin treatment should be stated on the albumin request form. In this study, only 1 patient (0.3%) had the duration of albumin treatment stated.
Another item on the albumin request form is the measurement of serum albumin levels 72 hours after starting albumin, which was not recorded for any of the 313 patients.
Discussion
The WHO uses a variety of intervention techniques, such as administrative, training, and monitoring measures, to encourage the prudent use of medications and enhance drug management programs. It is acknowledged that these strategies make medications more readily accessible within public health organizations, thereby helping low-income patients financially [8].
If medications are prescribed and used appropriately, more patients could be served and supported while keeping the limited medical budget in mind. As a result, it is critical to identify the costly but often prescribed drug productions and establish appropriate consumption patterns. DUE is a time-consuming process, but it has been effective in starting a discussion between physicians and pharmacists to achieve high standards for drug use in hospitals. It aids in revealing the drug administration patterns in the institutions under investigation [9].
Despite its high cost, albumin remains a commonly used medication. According to the most recent evidence-based research and recommendations [18], we assessed the appropriateness of albumin use.
In the present study, we evaluated the administration of albumin based on rational-use protocols, which provide an evidence-based assessment of prescribing by healthcare practitioners. Our study showed that albumin was used appropriately in 292 of 313 patients (93.2%).
Improper use of albumin results in significant resource waste and increases the likelihood of undesirable effects. DUEs can be used to identify patterns of albumin use in facilities, and the results could help physicians change their practices.
Because albumin and colloidal oncotic pressure are closely related, hypoalbuminemia may lead to or be the cause of edema [20]. Furthermore, a normal albumin level maintains a balance between the hydrostatic and colloid osmotic pressures inside vessels, preventing the development of edema [18]. Consequently, it is thought that albumin, which has diuretic and water-retention properties, can be used to treat edema caused by hypoalbuminemia [21, 22]. In our study, 2.3% of patients used the medication off-label during the research period.
Hypoalbuminemia was one of the most common reasons for albumin treatment in this analysis, accounting for 76 prescriptions (25.4%). A serum albumin concentration of less than 3.5–4 g/dL is known as hypoalbuminemia, and it is linked to several different clinical disorders [19]. Hypoalbuminemia has been linked to poor outcomes in different critical conditions [12, 20]. However, several studies have shown no discernible impact of albumin administration on mortality or morbidity in hypoalbuminemic patients [7]. Reduced serum albumin concentration alone is therefore not regarded as a good enough rationale for albumin replacement in several guidelines. Finding and treating the underlying causes of the hypoalbuminemia is a helpful practice for these patients.
On the other hand, some recommendations state that albumin should be administered only when the serum albumin level is less than 2.5 g/dL [22, 23]. In this study, 76 patients with an albumin level below 2.5 were candidates for receiving albumin vials. Approximately one-third of patients had serum albumin levels above the guideline cut-off (2.5 g/dL) at the time of albumin initiation, and in 3.6% of patients, this level was above 3.5 g/dL.
As noted above, the duration of albumin treatment should be stated on the albumin request form. In this study, only 1 patient (0.3%) had the duration of albumin treatment stated.
The measurement of serum albumin levels 72 hours after starting albumin is another item on the albumin request form, but none of the 313 patients had this information documented. It is crucial to monitor patients receiving albumin for 72 hours after the start of administration to assess ongoing need. Regretfully, this study found that no patients had this evaluation done after 72 hours. Patient monitoring and re-evaluation at least 72 hours after administration can minimize irrational drug administration and the associated financial burden, as the duration of albumin administration and the need for ongoing treatment vary by indication and patient factors [24].
In contrast to other studies, the most common improper use of albumin was observed after cardiac surgery in the studies by Jahangard-Rafsanjani et al. [25] and Kazemi et al. [5] at Shariati and Shaheed Rajaei hospitals in Tehran City, Iran. In addition, as in our investigation of irrational albumin utilization at Imam Reza Hospital in Tabriz City, Iran, Shafiee et al. [26] identified hypoalbuminemia and nutritional support as the most common causes.
A small number of studies examined the role of clinical pharmacists in optimizing albumin use, though most focused on developing albumin protocols [13, 27]. In addition to developing an approved protocol, Buckley et al. noted that clinical pharmacists assessed all albumin orders for appropriateness and intervened when necessary. In their report, inappropriate albumin consumption has significantly decreased by 72.9% [15]. According to Lyu et al. and Buckley et al. using established techniques resulted in an absolute decrease in albumin misuse of 50.9% and 36%, respectively [13, 15]. According to another study conducted in critically ill patients, the clinical pharmacists’ actions greatly improved the appropriateness of albumin usage in the ICU from 16.3% in the retrospective phase to 84.1% in the implementation phase [28]. Our study showed that the presence of an albumin prescription form in wards and pharmacist supervision were able to minimize irrational albumin prescriptions, at least in terms of inappropriate indications. However, the duration and need for continued treatment were not in compliance with the guideline, and we believe that the pharmacist’s attendance in the clinical wards could help minimize these errors. Given the financial burden and the local and even global shortage of albumin, greater pharmacist supervision of albumin request forms and compliance with guidelines can improve the rational prescribing and use of albumin.
This study represents a single teaching hospital site, and further research is needed to determine if these trends are present in other community hospital settings. The limitations of this study include the lack of investigation into the duration of albumin consumption and the total grams of albumin received by each patient, which should be examined more closely in future studies.
Conclusion
Hypoalbuminemia and ascites were the most common reasons for the administration of albumin. On the other hand, our study showed that the presence of an albumin prescription form in hospital wards and the presence of a pharmacist could minimize the irrational prescription of this drug. This study showed significant deviations from the albumin prescription protocol. Some aspects of albumin prescribing, including the minimum cut-off for starting albumin, the duration of use, and rechecking the albumin level, were not adequately considered by physicians. These findings emphasize a more sophisticated focus on the albumin prescribing in an attempt to minimize the irrational prescription of this expensive and valuable drug.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study design, and Final approval: All authors; Data collection and clinical studies: Ebrahim Salehifar, Zahra Bagherzadegan, and Shahram Ala; Data analysis and statistical analysis: Ebrahim Salehifar; Investigation and data acquisition: Sima Ramezaninejad; Writing the original draft: Sima Ramezaninejad; Review and editing: All authors; Supervision: Sima Ramezaninejad.
Conflict of interest
The authors declared no conflict of interest.
References
- Caraceni P, Domenicali M, Tovoli A, Napoli L, Ricci CS, Tufoni M, et al. Clinical indications for the albumin use: Still a controversial issue. Eur J Intern Med. 2013; 24(8):721-8. [DOI:10.1016/j.ejim.2013.05.015] [PMID]
- Mirici-Cappa F, Caraceni P, Domenicali M, Gelonesi E, Benazzi B, Zaccherini G, et al. How albumin administration for cirrhosis impacts on hospital albumin consumption and expenditure. World J Gastroenterol. 2011; 17(30):3479-86. [DOI:10.3748/wjg.v17.i30.3479] [PMID]
- Bachhav SS, Kshirsagar NA. Systematic review of drug utilization studies & the use of the drug classification system in the WHO-SEARO region. Indian J Med Res. 2015; 142(2):120-9. [DOI:10.4103/0971-5916.164223] [PMID]
- WHO. WHO medicines strategy: Framework for action in essential drugs and medicines policy 2000-2003. Geneva: WHO; 2000. [Link]
- Kazemi Y, Hadavand N, Hayatshahi A, Torkamandi H, Gholami K, Hadjibabaie M, et al. Albumin utilization in a teaching hospital in Tehran: Time to revise the prescribing strategies. J Pharm Care. 2015; 1(4):127-32. [Link]
- Rothschild MA, Oratz M, Schreiber SS. Serum albumin. Hepatology. 1988; 8(2):385-401. [DOI:10.1002/hep.1840080234] [PMID]
- Liumbruno GM, Bennardello F, Lattanzio A, Piccoli P, Rossettias G; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI). Recommendations for the use of albumin and immunoglobulins. Blood Transfus. 2009; 7(3):216-34. [DOI:10.2450/2009.0094-09] [PMID]
- Shahbazi Khamas S, Mirbagheri I, Dehnadi Moghadam A, Jafari A, Ashouri A. Evaluation of albumin utilization in a major teaching hospital in Iran before and after guideline implementation. J Pharm Care. 2021; 9(2):67-73. [Link]
- Javan-Noughabi J, Parnian E, Hajiesmaeili M, Salehiniya H, Setoodehzadeh F. The impact of a guideline to prevent inappropriate albumin administration in a hospital in Iran. Br J Heal Care Manag. 2020; 26(10):1-7. [Link]
- Zolfagharian F, Ghazanfari S, Elyasi S, Iraji P, Saberi MR, Vahdati-Mashhadian N, et al. Drug utilization evaluation of albumin in a teaching hospital of Mashhad, Iran: An interventional pre-post design study. Int J Clin Pharm. 2017; 39(4):704-11. [DOI:10.1007/s11096-017-0458-y] [PMID]
- Dastan F, Jamaati H, Emami H, Haghgoo R, Eskandari R, Hashemifard SS, et al. Reducing inappropriate utilization of albumin: the value of pharmacist-led intervention model. Iran J Pharm Res. 2018; 17(3):1125-9. [PMID]
- Farasatinasab M, Amouzegar A, Safari S, Ghanbari B, Darkahian M, Emami S, et al. Albumin utilization evaluation in a major teaching hospital in Iran: Recommendations for guideline development. J Res Pharm Pract. 2018; 7(3):157-63. [DOI:10.4103/jrpp.JRPP_18_4] [PMID]
- Lyu PF, Hockenberry JM, Gaydos LM, Howard DH, Buchman TG, Murphy DJ. Impact of a sequential intervention on albumin utilization in critical care. Crit Care Med. 2016; 44(7):1307-13. [DOI:10.1097/CCM.0000000000001638] [PMID]
- Ishida TS, Sakai MC, de Melo DO. The Appropriate use of human albumin in a Brazilian university hospital: Therapeutic indication and dosage regimen. Braz J Pharm Sci. 2018; 54 (4). [DOI:10.1590/s2175-97902018000418008]
- Buckley MS, Knutson KD, Agarwal SK, Lansburg JM, Wicks LM, Saggar RC, et al. Clinical pharmacist-led impact on inappropriate albumin use and costs in the critically Ill. Ann Pharmacother. 2020; 54(2):105-12. [DOI:10.1177/1060028019877471] [PMID]
- Chiatti C, Bustacchini S, Furneri G, Mantovani L, Cristiani M, Misuraca C, et al. The economic burden of inappropriate drug prescribing, lack of adherence and compliance, adverse drug events in older people: A systematic review. Drug Saf. 2012; 35(Suppl 1):73-87. [DOI:10.1007/BF03319105] [PMID]
- Noormandi A, Karimzadeh I, Mirjalili M, Khalili H. Clinical and economic impacts of clinical pharmacists' interventions in Iran: A systematic review. Daru. 2019; 27(1):361-78. [DOI:10.1007/s40199-019-00245-8] [PMID]
- Yu YT, Liu J, Hu B, Wang RL, Yang XH, Shang XL, et al. Expert consensus on the use of human serum albumin in critically ill patients. Chin Med J (Engl). 2021; 134(14):1639-54. [DOI:10.1097/CM9.0000000000001661] [PMID]
- Gatta A, Verardo A, Bolognesi M. Hypoalbuminemia. Intern Emerg Med. 2012; 7(Suppl 3):193-9. [DOI:10.1007/s11739-012-0802-0] [PMID]
- Margarson MP, Soni N. Serum albumin: Touchstone or totem? Anaesthesia. 1998; 53(8):789-803. [DOI:10.1046/j.1365-2044.1998.00438.x] [PMID]
- Aramwit P, Kasettratat N. Evaluation of serum albumin utilization in inpatient at a private hospital in Bangkok. Yakugaku Zasshi. 2004; 124(9):631-4. [DOI:10.1248/yakushi.124.631] [PMID]
- Talasaz AH, Jahangard-Rafsanjani Z, Ziaie S, Fahimi F. Evaluation of the pattern of human albumin utilization at a university affiliated hospital. Arch Iran Med. 2012; 15(2):85-7. [PMID]
- Delaney AP, Dan A, McCaffrey J, Finfer S. The role of albumin as a resuscitation fluid for patients with sepsis: A systematic review and meta-analysis. Crit Care Med. 2011; 39(2):386-91. [DOI:10.1097/CCM.0b013e3181ffe217] [PMID]
- Abedi F, Zarei B, Elyasi S. Albumin: A comprehensive review and practical guideline for clinical use. Eur J Clin Pharmacol. 2024; 80(8):1151-69. [DOI:10.1007/s00228-024-03664-y] [PMID]
- Jahangard‑Rafsanjani Z, Javadi MR, Torkamandi H, Alahyari S, Hajhossein Talasaz A, Gholami K, et al. The evaluation of albumin utilization in a teaching university hospital in Iran. Iran J Pharm Res. 2011; 10(2):385-90. [PMID]
- Shafiee E, Rezaee H, Entezari-Maleki T, Hamishehkar H. The evaluation of albumin use in an Iranian University hospital. Pharma Sci. 2016; 22(3):186–9. [DOI:10.15171/PS.2016.29]
- Farsad BF, Hadavand N, Masumi S, Salehi H. Albumin utilization review to evaluate the efficacy and cost, perform as a qualitative study in special wards in Shaheed Rajaei cardiovascular, medical &research center. Biosci Biotechnol Res Asia. 2016; 13(3):1469-77. [Link]
- Ibrahim DM, Shawki MA, Solayman MH, Sabri NA. The impact of clinical pharmacist implemented protocol on albumin utilization and cost in an Intensive Care Unit in Egypt. Front Pharmacol. 2022; 13:825048. [DOI:10.3389/fphar.2022.825048] [PMID]
Type of Study: Original Research |
Subject:
Clinical Pharmacy
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
