

Volume 11, Issue 3 (2025)
Pharm Biomed Res 2025, 11(3): 173-188 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezaee A, Rezaee M, Feyzabadi Z, Zarshenas M M. Clinical Applications of Myrtus communis L. in Traditional and Modern Medicine: A Scoping Review. Pharm Biomed Res 2025; 11 (3) :173-188
URL: http://pbr.mazums.ac.ir/article-1-697-en.html
URL: http://pbr.mazums.ac.ir/article-1-697-en.html



1- Student Research Committee, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
2- Student Research Committee, Faculty of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
3- Dr Feyzabadi Private Practice, Mashhad, Iran.
4- Department of Phytopharmaceuticals (Traditional Pharmacy), School of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran. & Medicinal Plants Processing Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
2- Student Research Committee, Faculty of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
3- Dr Feyzabadi Private Practice, Mashhad, Iran.
4- Department of Phytopharmaceuticals (Traditional Pharmacy), School of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran. & Medicinal Plants Processing Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
Full-Text [PDF 1258 kb]
(1761 Downloads)
| Abstract (HTML) (1614 Views)
Results
Properties of plants
MC, commonly known as myrtle, is an evergreen shrub, occasionally a small tree, native to the Mediterranean region. It reaches 2.4-3 m in height with branches forming a close full head [11]. The leaves are simple, opposite, and from ovate to lanceolate, measuring 2.5-3.8 cm long. They are dark green, shiny, glabrous, coriaceous, and aromatic. Leaf margins are whole, and leaves are opposite or verticillate. Flowers are solitary in the axil, on filiform peduncles. They are white with a diameter of approximately 2 cm, and others are yellow. The petals are glandular and pure white, with somewhat tomentose margins, covered with small hairs. A sweet fragrant smell comes from the flowers. The fruit is a small berry, pea-sized (0.7-1.2 cm), shaped orbicular or ovoid-ellipsoid. When ripened, it is blue-black or white. The berry is glabrous, of a rounded (vase-like) shape with the central part swollen and having remnants of persistent 4-5 partite calyx at the outer part. It is pale green at first, deep red after, and dark indigo when fully mature. They are bitter when unripe and sweet when ripe. Leaves and berries, which are widely used in traditional medicine, were collected. Figure 2 illustrates a visual representation of the plant [2].

Phytochemical compositions
The phytochemical compositions are presented in Table 1.
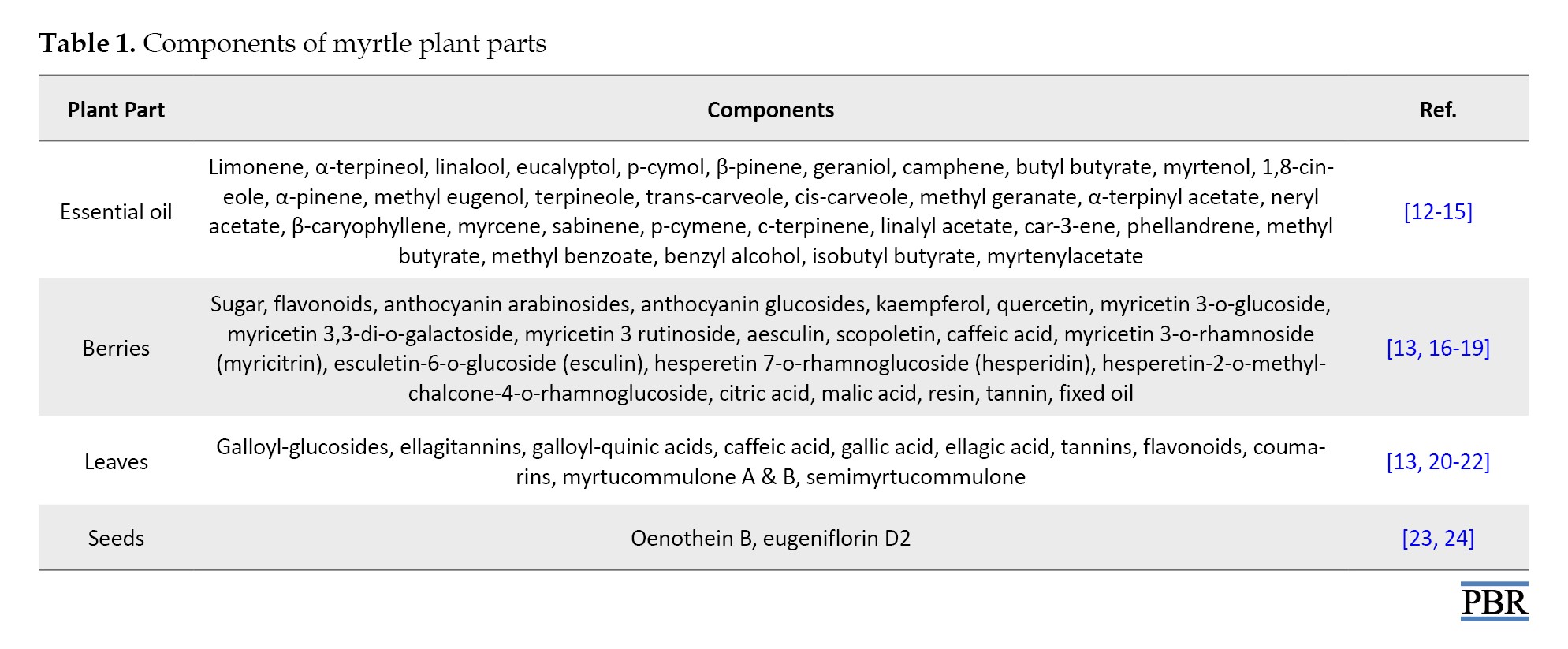
Table 1 summarizes detailed components.
Clinical applications from PM
Nature of MC in PM
PM physicians believed that the nature of MC is cold and dry because of two elements, water and soil. Coldness and astringency in the seeds, roots, and leaves are more pronounce than in other plant sections [4].
The history of MC
The use of myrtle to treat various diseases dates back thousands of years. The oldest known book on medicinal plants is “Materia Medica” (known as “Hashayesh” in Arabic), written by Pedanius Dioscorides (40 – 90 AD), a Greek physician and pharmacologist renowned as the father of botany. This work is considered the world’s first pharmacopeia and serves as an encyclopedia of herbal medicines. The name MC can be found in the Materia Medica [25].
Following Pedanius Dioscorides, eminent scientists such as Rhazes, and Avicenna. emerged from medical schools. These scholars expanded upon the knowledge of herbs, including MC, detailing their properties, such as temperament, habitat, indications, contraindications, duration of action, effectiveness, toxicity, dosage, types of preparations, and side effects [4].
Mode of application in PM
Neurological effects
Inhaling the aroma of myrtle leaves is recommended to treat headaches, dizziness, sinusitis, and epilepsy [4, 5].
Ophthalmic effects
A poultice prepared from barley and myrtle leaf extract is beneficial for treating pterygium, preventing tearing, and alleviating conjunctivitis [4, 5].
Ear, nose, and throat (ENT) and oral effects
MC is prescribed for toothache, earache, halitosis, oral lesions, mouth sores, epistaxis, hemoptysis, loose teeth, gingivitis, and tonsillitis. Applying the leaf extract inside the nose or ear is effective for epistaxis, ear pain, and ear discharge. Gargling with myrtle extract is beneficial for gingivitis, toothache, stuttering, and strengthening the gums [4].
Pulmonary effects
Myrtle syrup is beneficial for cough, hemoptysis, and tuberculosis [4, 5].
Gastrointestinal effect
MC extract acts as a tonic for the stomach and reduces nausea and vomiting. Myrtle syrup is effective for stomachache, heartburn, reflux, diarrhea, intestinal ulcers, mouth ulcers, and aphthous ulcers. Myrtle suppositories and sitting in a bath of boiled myrtle leaves are beneficial for anal prolapse, hemorrhoids, and intestinal worm infections. The smoke from burning myrtle leaves treats hemorrhoids [4].
Urogenital effects
MC syrup and suppositories are prescribed for heavy menstrual bleeding, uterine ulcers, warts, kidney stones, frequency, genital warts, and dysuria [4].
Dermatologic effects
Myrtle oil is useful for hair loss, dandruff, and acne. MC is used in various types of wounds and skin diseases in PM, such as deep, Purulent, chronic, and progressive wounds, burns, erysipelas, progressive blisters, pruritus, urticaria, and head and face skin lesions.
Body massaging with leaf powder in the bath strengthens the skin. Rubbing the leaves on the skin of warts causes them to disappear. Utilizing a dry leaf poultice on the armpits and groin areas eliminates unpleasant body sweat odor. Locally, myrtle leaves are used to removes dark spots on the face and bruises caused by trauma. An ointment from myrtle leaves and olive oil effectively treats burns [4].
Clinical applications from modern medicine
Dermatologic effects
The efficacy of the topical use of mixed 1x MC leaves processed with 2x water and oral 4.5 g Descurainia Sophia L. was nearly twice than the salicylic acid (16.5%) group, the MC alone group, and the combined salicylic acid and D. Sophia group in terms of wart size and number reduction on days 40 and 90. No wart relapse was reported in any group. The combined MC and D. Sophia group had fewer side effects than the salicylic acid group [26].
A dermo-cosmetic cream containing azelaic acid and MC leaves reduced acne relapse by 18% compared to a light moisturizing cream at week 16. However, it was not statistically significant, probably due to the small sample size [27]. The use of topically applied myrtle leaves significantly decreased comedones, acne severity index, and total lesion count compared to the clindamycin group. The myrtle and clindamycin groups showed similar reductions in inflammatory lesions [28]. In a clinical trial, MC leaf cream was administered to 100 nulliparous women after episiotomy for wound healing evaluation. The Reeda score (edema, erythema, exudation, and bruising) was significantly reduced on days 5 and 10 in the MC leaves cream group compared to the placebo group [29].
MC leaves solution was as effective as ketoconazole shampoo for dandruff treatment. While the difference between the two groups was not statistically significant, both treatments significantly reduced excoriation pruritus grading, adherent scalp flaking score, redness of scalp skin, and grading of scalp skin involvement [30]. Itching and erythema were reported as adverse effects of 2% ketoconazole shampoo [31]. No side effects have been reported for myrtle. Therefore, myrtle may be more effective than ketoconazole shampoo for dandruff treatment.
Gastrointestinal effect
It was demonstrated that the essential oil from myrtle leaves in the ointment could significantly decrease anal itching compared to the anti-hemorrhoid drug group in postpartum women with grade I and II internal hemorrhoids at week 8. Pain, itching, swelling, bleeding, and discomfort in the anus were reduced within both myrtle and anti-hemorrhoid drug groups, similar to each other [32]. The effects of the MC freeze-dried aqueous extract capsule, omeprazole, and a combination of omeprazole and the MC capsule were evaluated in adults with GERD at 6 weeks. All three interventions were effective on acid reflux-related symptoms (RS), dysmotility-like symptoms (DS), and scores of frequency scale for the symptoms of gastroesophageal reflux disease (GERD) within group comparisons. Between-group comparisons showed similar efficacy. Although all interventions were significant, the FSSG and reflux-related symptoms (RS) mean differences of the omeprazole group were reported to be the highest, while the dysmotility-like symptoms (DS) mean difference of the omeprazole and MC capsule combination was shown to be the largest [33]. A clinical trial on children showed no differences in GERD symptom questionnaire scores for young children between the combination of MC fruit syrup and omeprazole and omeprazole alone in weeks 8 and 12. However, children in the myrtle group experienced a significant increase in appetite [34]. An in vivo study demonstrated that a-tocopherol and flavonoids protect against mucosal damage in rats with GERD via antioxidative activities. Notably, flavonoids are found in myrtle [13, 35].
Urogenital effects
The efficacy of MC and oak gall vaginal suppositories (MOGS) compared to the placebo and metronidazole groups in women with vaginitis was assessed. Metronidazole was more effective in reducing malodor discharge, malodor discharge after intercourse, dyspareunia, vaginal irritation, dysuria, lower abdominal pain, Whiff test-positivity, clue cells-presence, Candida albicans-presence, Gardnerella-presence, Trichomonas-presence than the MOGS and placebo groups. However, MOGS was more effective in relieving itching than other groups. In both trichomoniasis vaginosis (TV) and bacterial vaginosis (BV) patients, MOGS treatment resulted in a greater mean difference in discharge, although not statistically significant. The Nugent score and trichomoniasis vaginosis (TV) significantly decreased in both MOGS and metronidazole groups, while BV was reduced considerably only in the metronidazole group [36]. In another clinical trial, BV was assessed among women with BV on day 7. Metronidazole alone was more effective against BV than MC in a metronidazole base and Berberis vulgaris in a metronidazole base, although relapse was reported as zero in the MC and B. vulgaris groups as opposed to the metronidazole group [37].
The efficacy of 15 mL of MC fruit syrup was evaluated in women with excessive uterine bleeding. In month 3, the results reported a marked reduction in the mean pad number, mean bleeding days, and MQ score [38]. Another study administering 750 mg MC fruit capsules to women with menorrhagia for 10 days in two cycles demonstrated a significant reduction in pictorial blood loss assessment chart (PBAC) scores and a considerable increase in quality of life and hemoglobin percentage after the second cycle of treatment compared to the control group [39].
A 3-month study was conducted to evaluate human papillomavirus (HPV) test circumstances in women with cervicovaginal HPV infection. Vaginal suppositories containing 0.5% MC leaf essential oil, and 10% MC leaf aqueous extract and placebos were administered. The HPV test was significantly negative in the MC group compared to the placebo group, and as a result, the cervical lesion size decreased considerably [40].
In women with vulvovaginal candidiasis, Ward preparation (containing Quercus infectoria, Rosa damascena, Nardostachys jatamansi, MC, and Punica granatum) markedly decreased symptoms, including itching, vaginal edema, dyspareunia, vaginal discharge, and vaginal redness compared to the placebo group after five weeks of treatment [41].
A study on nulliparous women after an episiotomy procedure showed that MC cream considerably reduced pain severity at 5- and 10-hours post-procedure compared to the placebo group [29].
ENT and oral effects
A before-and-after clinical trial was conducted on patients with epistaxis, nasal erosion, and mucosal dryness administering an intranasal spray mixture containing anthocyanin, fucoidan, hyaluronic acid, and MC. At week 8, endoscopic examination showed a remarkable reduction in epistaxis, nasal erosion, and mucosal dryness, compared to baseline [42].
The efficacy of MC oral paste in patients with recurrent aphthous stomatitis (RAS) demonstrated significant reductions in ulcer size, pain sensitivity, erythema, and exudation [43].
A clustered clinical trial assessed the efficacy of 4 essential oil mixtures vaporization, containing Citrus aurantifolia, Citrus limon, Osmanthus fragrance, Citrus sinensis; forest walk (FW): Containing MC, Pinus cembra, A. sibirica, A. grandis, Vetiveria zizanoides, Citrus paradisi, Abies alba, Pseudotsuga menziesii; Swiss pine (SP): Containing P. cembra compared to the control group on acute anxiety. Acute anxiety, as measured by the state-trait-anxiety inventory (STAI-T), was significantly reduced in all intervention groups compared to the control group, particularly in women [44].
Table 2 summarizes the characteristics of the 17 included clinical trials.
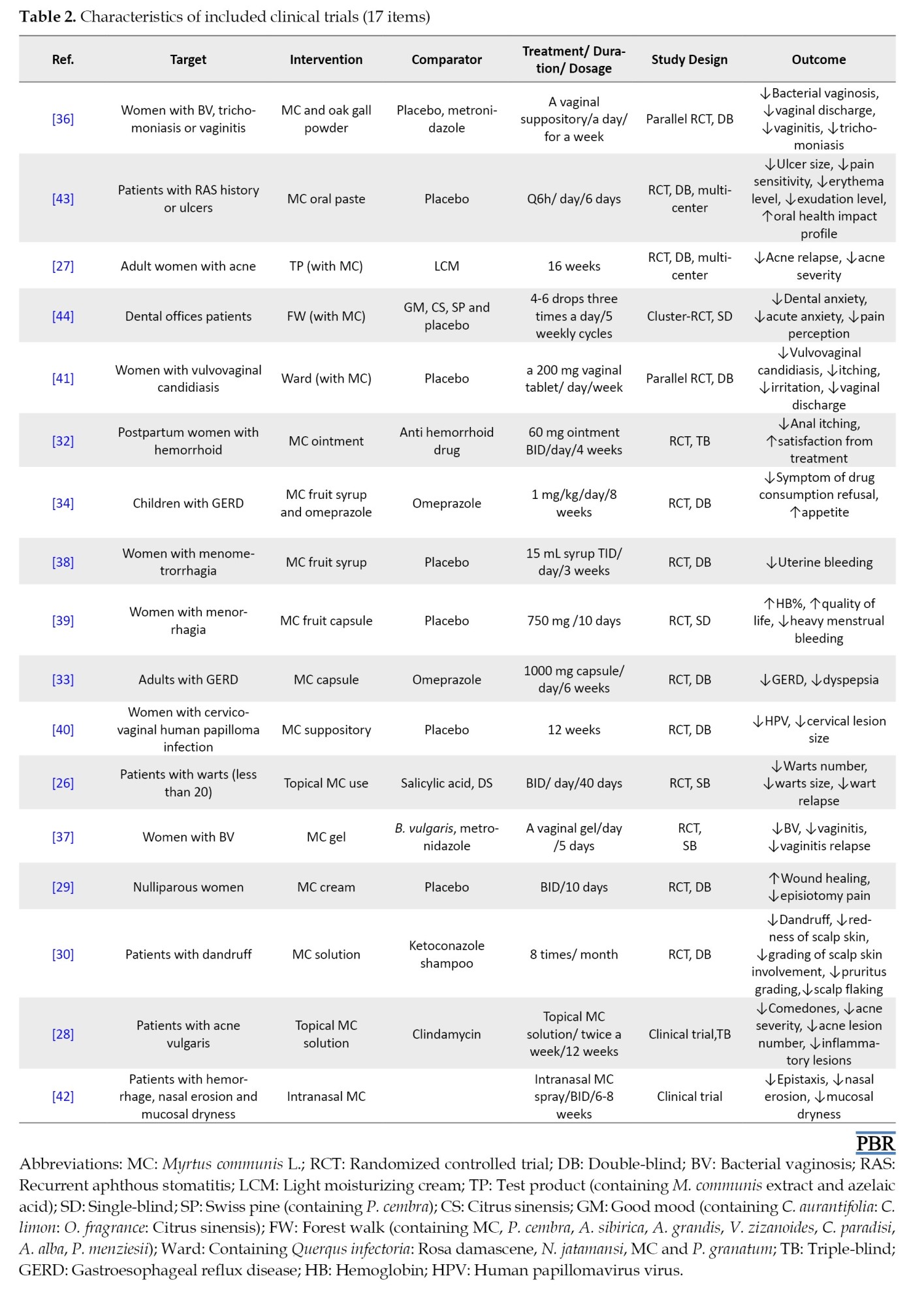
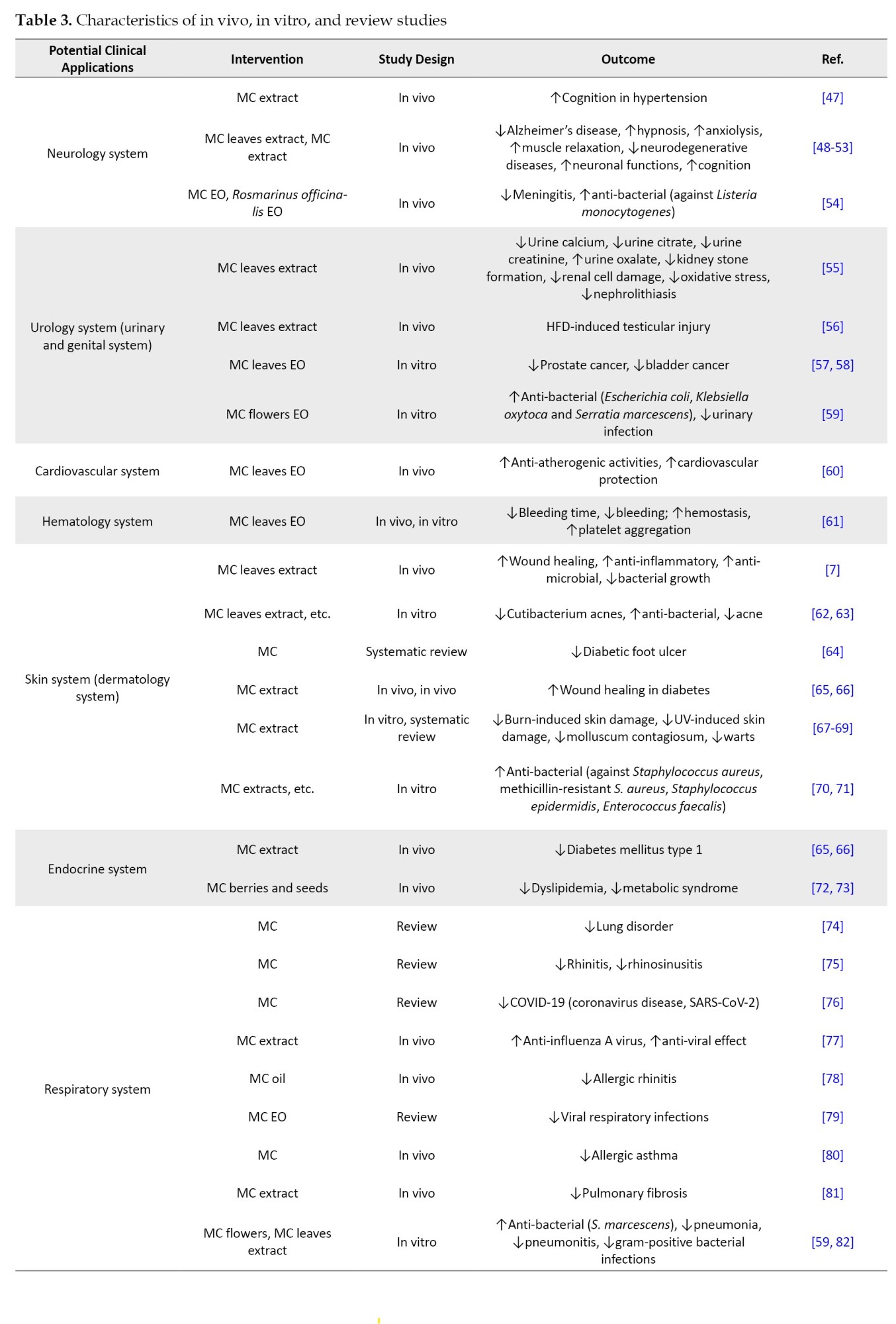
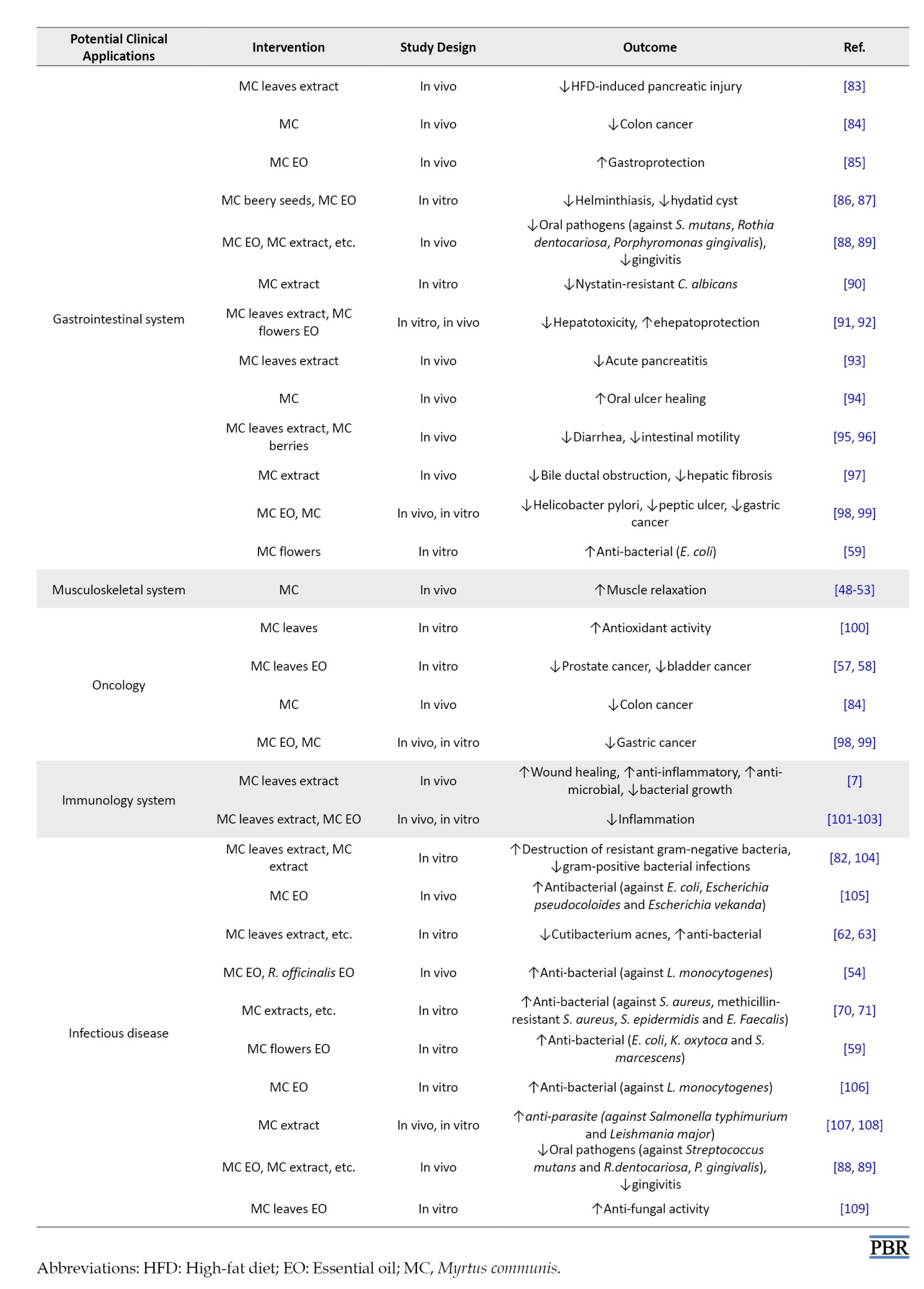
Table 3 presents the potential in vivo and in vitro applications.
Potential clinical applications from in vivo and in vitro studies
Due to the myrtle’s various yet unexplored medical applications, we have summarized in vivo and in vitro studies regarding myrtle in Table 3. These findings may inform future clinical trials.
Side effects and toxicity
The efficacy of a 4% myrtle leaves diet on sheep was evaluated. The study showed a considerable decrease in triglyceride and blood sugar. While this effect has not been reported in humans, it suggests the potential for similar outcomes in human subjects [45]. Additionally, the LD50 values (median lethal dose) of aqueous and ethanolic myrtle extracts were reported as 0.473 and 0.79 g/kg, respectively [46]. High cineole content in MC can cause hypotension and respiratory failure [2].
Discussion
In this review article, for the first time, the myrtle plant has been evaluated from the perspective of temperament and humoral medicine. The properties of this plant have been explained based on its temperament in the oldest books of traditional Persian and Greek medicine, such as “Materia Medica” (known as “Hashayesh” in Arabic), by Pedanius Dioscorides and The Canon of Medicine by Avicenna.
Alipour et al. (2014) examined the mechanisms of various activities of this plant [6], and Hennia et al. in 2018 examined its antioxidant activity [13].
This article reviewed for the first time the therapeutic applications and methods of oral and topical use of myrtle plants in traditional medicine books and compared them with the results of modern clinical studies. However, other review articles have only mentioned the therapeutic effects of myrtle in scientific studies, along with the plant’s pharmacology and mechanism of action [6, 10, 13].
One of our article’s strengths is the review of the therapeutic uses of myrtle in traditional medicine books from thousands of years ago to the present, based on human, animal, and laboratory studies. One of our article’s weaknesses is the less thorough review of the mechanism of myrtle’s pharmacological effects.
Conclusion
Herbal medicines have been extensively used in PM. Some MC applications in PM have been proven by modern medicine, while others remain unproven. Many potential uses were conducted in in vivo and in vitro studies; therefore, they have the potential to be conducted in future clinical trials. MC contains crucial bioactive components, including anthraquinones, phenolics, flavonoids, tannins, saponosides, coumarins, quinones, and alkaloids. These compounds suggest potential applications in treating neurological, urogenital, gastrointestinal, dermatological, and otorhinolaryngological diseases.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Mohsen Rezaee and Ali Rezaee; Methodology: All authors; Writing the original draft: Ali Rezaee; Review and editing: Zohre Feyzabadi and Mohammad M. Zarshenas.
Conflict of interest
The authors declared no conflict of interest.
References
Full-Text: (1565 Views)
Introduction
Myrtus communis L. (MC), commonly known as myrtle, belongs to the Myrtaceae family. It grows spontaneously as an evergreen bush or small tree, native to the coastal areas of the Mediterranean regions, North Africa, and Southern Europe. The plant has also spread to South America, Australia, and Iran [1]. In Persian medicine (PM), the plant is referred to as Mord or Habb-ul-Aas. According to the morphology in the book “matching the old medicinal plant name with scientific terminology” by two Iranian botanists, these names correspond to MC [2, 3]. MC has been widely used to treat various conditions, including gastroesophageal reflux disease (GERD), cough, palpitation, dysuria, stress incontinence, anogenital and common warts, acne, and homeostasis, such as epistaxis, hemoptysis, uterine bleeding, hemorrhoids, and ulcers in PM. Similar to Unani medicine, PM is a traditional medical system based on humoral medicine, with rich literature on medicinal plants properties and their therapeutic applications. In PM, everything is believed to have a temperament based on four elementary properties (warmth, moisture, dryness, and coldness) [4, 5]. Plants also have temperaments. Temperaments are determined by the plant’s actions, smell, taste, and color. PM scholars attribute a cold and dry nature to MC, making it widely used in illnesses with warm dystemperament [4].
In modern medicine, MC has been reported to possess hemostatic, anti-inflammatory, analgesic, antioxidant, antiviral, antibacterial, and cytotoxic activities [6-8]. The essential oil of MC from Benslimane region contains high percentages of geranyl acetate (11.64%), α-terpineol (15.5%), and methyl eugenol (18.7%) in gas chromatography–mass spectrometry analyses from Benslimane region [9] The plant has also been revealed to contain anthraquinones, phenolics, flavonoids, tannins, saponosides, coumarins, quinones, and alkaloids [10].
This review aimed to assess the pharmacological properties, adverse events, toxicity, and clinical applications of MC based on both modern research and PM, and beneficial clinical applications may be provided for future clinical trials.
Materials and Methods
In this review, the clinical and medicinal properties of MC were extracted from Iranian PhD students’ PM textbooks. Famous pharmaceutical and medical textbooks taught at schools of traditional medicine in Iran, including ‘the canon of medicine’ and ‘makhzan al-adviyah’, were consulted for PM [4, 5]. In the references, sections relating to the therapeutic, appearance, habitat properties, and pharmaceutical products of common myrtle (Mord or Habb-ul-Aas) were assessed, and associated data were included and classified.
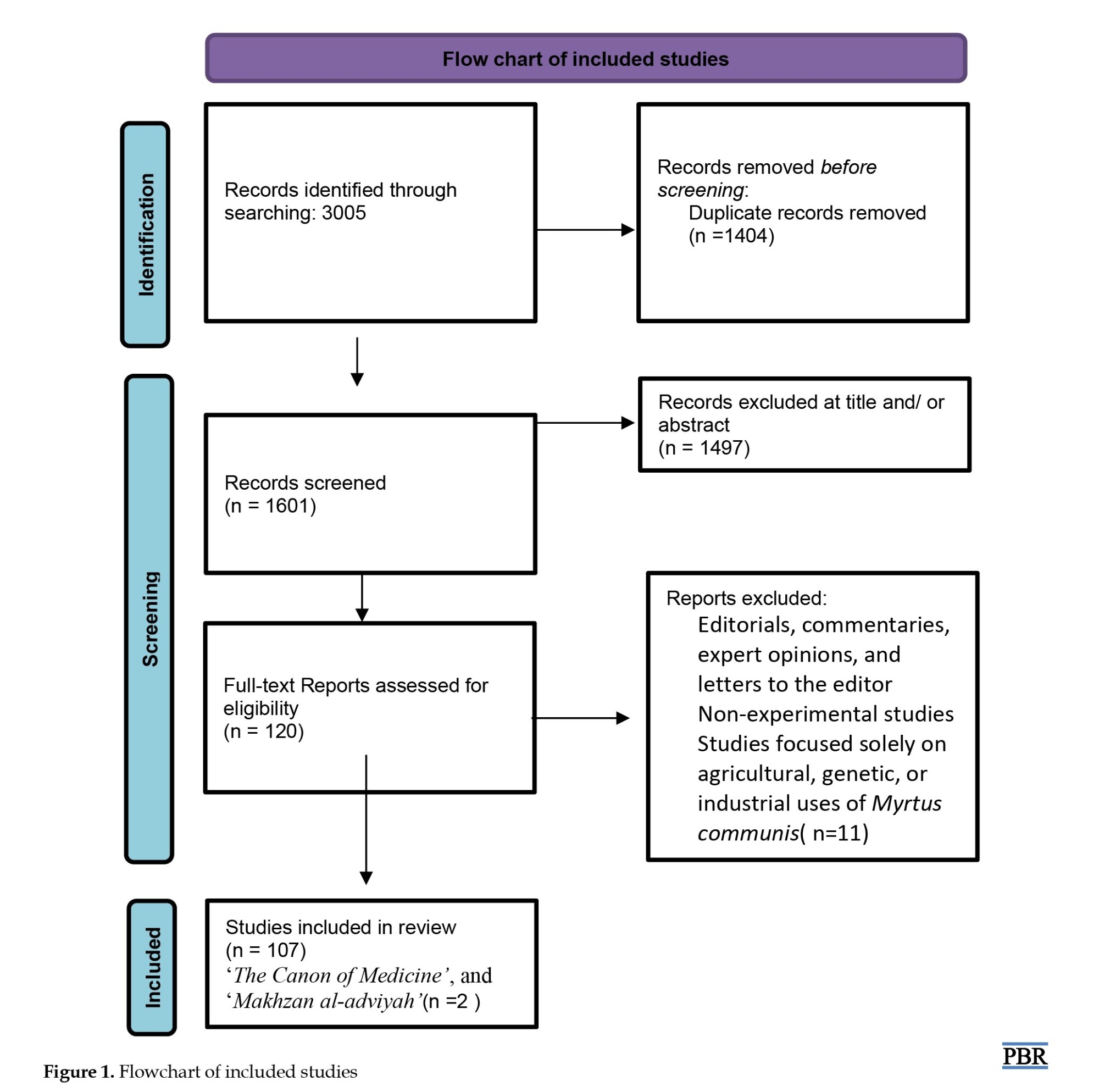
For modern medicine, the search was conducted through scientific databases, including ScienceDirect, Scopus, Embase, and PubMed, using ‘common myrtle’, ‘Myrtus communis’, and ‘Myrtus communis L.’ as keywords among abstracts, titles, and keywords parts of databases. All associated clinical trials, in vivo, and in vitro studies that may have clinical applications from the beginning to June 2024 were included. Whole letters, conference articles, and articles related to the genetics and agriculture of common myrtle were excluded. Figure 1 illustrates this selection process.
Myrtus communis L. (MC), commonly known as myrtle, belongs to the Myrtaceae family. It grows spontaneously as an evergreen bush or small tree, native to the coastal areas of the Mediterranean regions, North Africa, and Southern Europe. The plant has also spread to South America, Australia, and Iran [1]. In Persian medicine (PM), the plant is referred to as Mord or Habb-ul-Aas. According to the morphology in the book “matching the old medicinal plant name with scientific terminology” by two Iranian botanists, these names correspond to MC [2, 3]. MC has been widely used to treat various conditions, including gastroesophageal reflux disease (GERD), cough, palpitation, dysuria, stress incontinence, anogenital and common warts, acne, and homeostasis, such as epistaxis, hemoptysis, uterine bleeding, hemorrhoids, and ulcers in PM. Similar to Unani medicine, PM is a traditional medical system based on humoral medicine, with rich literature on medicinal plants properties and their therapeutic applications. In PM, everything is believed to have a temperament based on four elementary properties (warmth, moisture, dryness, and coldness) [4, 5]. Plants also have temperaments. Temperaments are determined by the plant’s actions, smell, taste, and color. PM scholars attribute a cold and dry nature to MC, making it widely used in illnesses with warm dystemperament [4].
In modern medicine, MC has been reported to possess hemostatic, anti-inflammatory, analgesic, antioxidant, antiviral, antibacterial, and cytotoxic activities [6-8]. The essential oil of MC from Benslimane region contains high percentages of geranyl acetate (11.64%), α-terpineol (15.5%), and methyl eugenol (18.7%) in gas chromatography–mass spectrometry analyses from Benslimane region [9] The plant has also been revealed to contain anthraquinones, phenolics, flavonoids, tannins, saponosides, coumarins, quinones, and alkaloids [10].
This review aimed to assess the pharmacological properties, adverse events, toxicity, and clinical applications of MC based on both modern research and PM, and beneficial clinical applications may be provided for future clinical trials.
Materials and Methods
In this review, the clinical and medicinal properties of MC were extracted from Iranian PhD students’ PM textbooks. Famous pharmaceutical and medical textbooks taught at schools of traditional medicine in Iran, including ‘the canon of medicine’ and ‘makhzan al-adviyah’, were consulted for PM [4, 5]. In the references, sections relating to the therapeutic, appearance, habitat properties, and pharmaceutical products of common myrtle (Mord or Habb-ul-Aas) were assessed, and associated data were included and classified.
For modern medicine, the search was conducted through scientific databases, including ScienceDirect, Scopus, Embase, and PubMed, using ‘common myrtle’, ‘Myrtus communis’, and ‘Myrtus communis L.’ as keywords among abstracts, titles, and keywords parts of databases. All associated clinical trials, in vivo, and in vitro studies that may have clinical applications from the beginning to June 2024 were included. Whole letters, conference articles, and articles related to the genetics and agriculture of common myrtle were excluded. Figure 1 illustrates this selection process.
Results
Properties of plants
MC, commonly known as myrtle, is an evergreen shrub, occasionally a small tree, native to the Mediterranean region. It reaches 2.4-3 m in height with branches forming a close full head [11]. The leaves are simple, opposite, and from ovate to lanceolate, measuring 2.5-3.8 cm long. They are dark green, shiny, glabrous, coriaceous, and aromatic. Leaf margins are whole, and leaves are opposite or verticillate. Flowers are solitary in the axil, on filiform peduncles. They are white with a diameter of approximately 2 cm, and others are yellow. The petals are glandular and pure white, with somewhat tomentose margins, covered with small hairs. A sweet fragrant smell comes from the flowers. The fruit is a small berry, pea-sized (0.7-1.2 cm), shaped orbicular or ovoid-ellipsoid. When ripened, it is blue-black or white. The berry is glabrous, of a rounded (vase-like) shape with the central part swollen and having remnants of persistent 4-5 partite calyx at the outer part. It is pale green at first, deep red after, and dark indigo when fully mature. They are bitter when unripe and sweet when ripe. Leaves and berries, which are widely used in traditional medicine, were collected. Figure 2 illustrates a visual representation of the plant [2].
Phytochemical compositions
The phytochemical compositions are presented in Table 1.
Table 1 summarizes detailed components.
Clinical applications from PM
Nature of MC in PM
PM physicians believed that the nature of MC is cold and dry because of two elements, water and soil. Coldness and astringency in the seeds, roots, and leaves are more pronounce than in other plant sections [4].
The history of MC
The use of myrtle to treat various diseases dates back thousands of years. The oldest known book on medicinal plants is “Materia Medica” (known as “Hashayesh” in Arabic), written by Pedanius Dioscorides (40 – 90 AD), a Greek physician and pharmacologist renowned as the father of botany. This work is considered the world’s first pharmacopeia and serves as an encyclopedia of herbal medicines. The name MC can be found in the Materia Medica [25].
Following Pedanius Dioscorides, eminent scientists such as Rhazes, and Avicenna. emerged from medical schools. These scholars expanded upon the knowledge of herbs, including MC, detailing their properties, such as temperament, habitat, indications, contraindications, duration of action, effectiveness, toxicity, dosage, types of preparations, and side effects [4].
Mode of application in PM
Neurological effects
Inhaling the aroma of myrtle leaves is recommended to treat headaches, dizziness, sinusitis, and epilepsy [4, 5].
Ophthalmic effects
A poultice prepared from barley and myrtle leaf extract is beneficial for treating pterygium, preventing tearing, and alleviating conjunctivitis [4, 5].
Ear, nose, and throat (ENT) and oral effects
MC is prescribed for toothache, earache, halitosis, oral lesions, mouth sores, epistaxis, hemoptysis, loose teeth, gingivitis, and tonsillitis. Applying the leaf extract inside the nose or ear is effective for epistaxis, ear pain, and ear discharge. Gargling with myrtle extract is beneficial for gingivitis, toothache, stuttering, and strengthening the gums [4].
Pulmonary effects
Myrtle syrup is beneficial for cough, hemoptysis, and tuberculosis [4, 5].
Gastrointestinal effect
MC extract acts as a tonic for the stomach and reduces nausea and vomiting. Myrtle syrup is effective for stomachache, heartburn, reflux, diarrhea, intestinal ulcers, mouth ulcers, and aphthous ulcers. Myrtle suppositories and sitting in a bath of boiled myrtle leaves are beneficial for anal prolapse, hemorrhoids, and intestinal worm infections. The smoke from burning myrtle leaves treats hemorrhoids [4].
Urogenital effects
MC syrup and suppositories are prescribed for heavy menstrual bleeding, uterine ulcers, warts, kidney stones, frequency, genital warts, and dysuria [4].
Dermatologic effects
Myrtle oil is useful for hair loss, dandruff, and acne. MC is used in various types of wounds and skin diseases in PM, such as deep, Purulent, chronic, and progressive wounds, burns, erysipelas, progressive blisters, pruritus, urticaria, and head and face skin lesions.
Body massaging with leaf powder in the bath strengthens the skin. Rubbing the leaves on the skin of warts causes them to disappear. Utilizing a dry leaf poultice on the armpits and groin areas eliminates unpleasant body sweat odor. Locally, myrtle leaves are used to removes dark spots on the face and bruises caused by trauma. An ointment from myrtle leaves and olive oil effectively treats burns [4].
Clinical applications from modern medicine
Dermatologic effects
The efficacy of the topical use of mixed 1x MC leaves processed with 2x water and oral 4.5 g Descurainia Sophia L. was nearly twice than the salicylic acid (16.5%) group, the MC alone group, and the combined salicylic acid and D. Sophia group in terms of wart size and number reduction on days 40 and 90. No wart relapse was reported in any group. The combined MC and D. Sophia group had fewer side effects than the salicylic acid group [26].
A dermo-cosmetic cream containing azelaic acid and MC leaves reduced acne relapse by 18% compared to a light moisturizing cream at week 16. However, it was not statistically significant, probably due to the small sample size [27]. The use of topically applied myrtle leaves significantly decreased comedones, acne severity index, and total lesion count compared to the clindamycin group. The myrtle and clindamycin groups showed similar reductions in inflammatory lesions [28]. In a clinical trial, MC leaf cream was administered to 100 nulliparous women after episiotomy for wound healing evaluation. The Reeda score (edema, erythema, exudation, and bruising) was significantly reduced on days 5 and 10 in the MC leaves cream group compared to the placebo group [29].
MC leaves solution was as effective as ketoconazole shampoo for dandruff treatment. While the difference between the two groups was not statistically significant, both treatments significantly reduced excoriation pruritus grading, adherent scalp flaking score, redness of scalp skin, and grading of scalp skin involvement [30]. Itching and erythema were reported as adverse effects of 2% ketoconazole shampoo [31]. No side effects have been reported for myrtle. Therefore, myrtle may be more effective than ketoconazole shampoo for dandruff treatment.
Gastrointestinal effect
It was demonstrated that the essential oil from myrtle leaves in the ointment could significantly decrease anal itching compared to the anti-hemorrhoid drug group in postpartum women with grade I and II internal hemorrhoids at week 8. Pain, itching, swelling, bleeding, and discomfort in the anus were reduced within both myrtle and anti-hemorrhoid drug groups, similar to each other [32]. The effects of the MC freeze-dried aqueous extract capsule, omeprazole, and a combination of omeprazole and the MC capsule were evaluated in adults with GERD at 6 weeks. All three interventions were effective on acid reflux-related symptoms (RS), dysmotility-like symptoms (DS), and scores of frequency scale for the symptoms of gastroesophageal reflux disease (GERD) within group comparisons. Between-group comparisons showed similar efficacy. Although all interventions were significant, the FSSG and reflux-related symptoms (RS) mean differences of the omeprazole group were reported to be the highest, while the dysmotility-like symptoms (DS) mean difference of the omeprazole and MC capsule combination was shown to be the largest [33]. A clinical trial on children showed no differences in GERD symptom questionnaire scores for young children between the combination of MC fruit syrup and omeprazole and omeprazole alone in weeks 8 and 12. However, children in the myrtle group experienced a significant increase in appetite [34]. An in vivo study demonstrated that a-tocopherol and flavonoids protect against mucosal damage in rats with GERD via antioxidative activities. Notably, flavonoids are found in myrtle [13, 35].
Urogenital effects
The efficacy of MC and oak gall vaginal suppositories (MOGS) compared to the placebo and metronidazole groups in women with vaginitis was assessed. Metronidazole was more effective in reducing malodor discharge, malodor discharge after intercourse, dyspareunia, vaginal irritation, dysuria, lower abdominal pain, Whiff test-positivity, clue cells-presence, Candida albicans-presence, Gardnerella-presence, Trichomonas-presence than the MOGS and placebo groups. However, MOGS was more effective in relieving itching than other groups. In both trichomoniasis vaginosis (TV) and bacterial vaginosis (BV) patients, MOGS treatment resulted in a greater mean difference in discharge, although not statistically significant. The Nugent score and trichomoniasis vaginosis (TV) significantly decreased in both MOGS and metronidazole groups, while BV was reduced considerably only in the metronidazole group [36]. In another clinical trial, BV was assessed among women with BV on day 7. Metronidazole alone was more effective against BV than MC in a metronidazole base and Berberis vulgaris in a metronidazole base, although relapse was reported as zero in the MC and B. vulgaris groups as opposed to the metronidazole group [37].
The efficacy of 15 mL of MC fruit syrup was evaluated in women with excessive uterine bleeding. In month 3, the results reported a marked reduction in the mean pad number, mean bleeding days, and MQ score [38]. Another study administering 750 mg MC fruit capsules to women with menorrhagia for 10 days in two cycles demonstrated a significant reduction in pictorial blood loss assessment chart (PBAC) scores and a considerable increase in quality of life and hemoglobin percentage after the second cycle of treatment compared to the control group [39].
A 3-month study was conducted to evaluate human papillomavirus (HPV) test circumstances in women with cervicovaginal HPV infection. Vaginal suppositories containing 0.5% MC leaf essential oil, and 10% MC leaf aqueous extract and placebos were administered. The HPV test was significantly negative in the MC group compared to the placebo group, and as a result, the cervical lesion size decreased considerably [40].
In women with vulvovaginal candidiasis, Ward preparation (containing Quercus infectoria, Rosa damascena, Nardostachys jatamansi, MC, and Punica granatum) markedly decreased symptoms, including itching, vaginal edema, dyspareunia, vaginal discharge, and vaginal redness compared to the placebo group after five weeks of treatment [41].
A study on nulliparous women after an episiotomy procedure showed that MC cream considerably reduced pain severity at 5- and 10-hours post-procedure compared to the placebo group [29].
ENT and oral effects
A before-and-after clinical trial was conducted on patients with epistaxis, nasal erosion, and mucosal dryness administering an intranasal spray mixture containing anthocyanin, fucoidan, hyaluronic acid, and MC. At week 8, endoscopic examination showed a remarkable reduction in epistaxis, nasal erosion, and mucosal dryness, compared to baseline [42].
The efficacy of MC oral paste in patients with recurrent aphthous stomatitis (RAS) demonstrated significant reductions in ulcer size, pain sensitivity, erythema, and exudation [43].
A clustered clinical trial assessed the efficacy of 4 essential oil mixtures vaporization, containing Citrus aurantifolia, Citrus limon, Osmanthus fragrance, Citrus sinensis; forest walk (FW): Containing MC, Pinus cembra, A. sibirica, A. grandis, Vetiveria zizanoides, Citrus paradisi, Abies alba, Pseudotsuga menziesii; Swiss pine (SP): Containing P. cembra compared to the control group on acute anxiety. Acute anxiety, as measured by the state-trait-anxiety inventory (STAI-T), was significantly reduced in all intervention groups compared to the control group, particularly in women [44].
Table 2 summarizes the characteristics of the 17 included clinical trials.
Table 3 presents the potential in vivo and in vitro applications.
Potential clinical applications from in vivo and in vitro studies
Due to the myrtle’s various yet unexplored medical applications, we have summarized in vivo and in vitro studies regarding myrtle in Table 3. These findings may inform future clinical trials.
Side effects and toxicity
The efficacy of a 4% myrtle leaves diet on sheep was evaluated. The study showed a considerable decrease in triglyceride and blood sugar. While this effect has not been reported in humans, it suggests the potential for similar outcomes in human subjects [45]. Additionally, the LD50 values (median lethal dose) of aqueous and ethanolic myrtle extracts were reported as 0.473 and 0.79 g/kg, respectively [46]. High cineole content in MC can cause hypotension and respiratory failure [2].
Discussion
In this review article, for the first time, the myrtle plant has been evaluated from the perspective of temperament and humoral medicine. The properties of this plant have been explained based on its temperament in the oldest books of traditional Persian and Greek medicine, such as “Materia Medica” (known as “Hashayesh” in Arabic), by Pedanius Dioscorides and The Canon of Medicine by Avicenna.
Alipour et al. (2014) examined the mechanisms of various activities of this plant [6], and Hennia et al. in 2018 examined its antioxidant activity [13].
This article reviewed for the first time the therapeutic applications and methods of oral and topical use of myrtle plants in traditional medicine books and compared them with the results of modern clinical studies. However, other review articles have only mentioned the therapeutic effects of myrtle in scientific studies, along with the plant’s pharmacology and mechanism of action [6, 10, 13].
One of our article’s strengths is the review of the therapeutic uses of myrtle in traditional medicine books from thousands of years ago to the present, based on human, animal, and laboratory studies. One of our article’s weaknesses is the less thorough review of the mechanism of myrtle’s pharmacological effects.
Conclusion
Herbal medicines have been extensively used in PM. Some MC applications in PM have been proven by modern medicine, while others remain unproven. Many potential uses were conducted in in vivo and in vitro studies; therefore, they have the potential to be conducted in future clinical trials. MC contains crucial bioactive components, including anthraquinones, phenolics, flavonoids, tannins, saponosides, coumarins, quinones, and alkaloids. These compounds suggest potential applications in treating neurological, urogenital, gastrointestinal, dermatological, and otorhinolaryngological diseases.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Mohsen Rezaee and Ali Rezaee; Methodology: All authors; Writing the original draft: Ali Rezaee; Review and editing: Zohre Feyzabadi and Mohammad M. Zarshenas.
Conflict of interest
The authors declared no conflict of interest.
References
- Özkan AM, Güray ÇG. A Mediterranean: Myrtus communis L.(myrtle). In: Morel JP, Mercuri AM (editors). Plants and culture: Seeds of the cultural heritage of Europe. Bari: Edipuglia: 2009. [Link]
- Emami A, Mehregan I, Fasihi Sh. [Medicinal plants reference book (Persian)]. Tehran: Andisheh-e-Noor Publishing; 2010. [Link]
- Ghahreman A, Okhovvat AR. [Matching the old medicinal plant names with scientific terminology (Persian)]. Tehran: University of Tehran Press; 2010. [Link]
- Avicenna. The Canon of medicine. [F. Esmaieli (Persian trans]. Tehran: Kahkeshane Elm; 2024. [Link]
- Aghili Alavi Khorasani Shirazi MH. [Makhzan al-Advieh (Persian)]. Tehran: Chogan; 2014. [Link]
- Alipour G, Dashti S, Hosseinzadeh H. Review of pharmacological effects of Myrtus communis L. and its active constituents. Phytother Res. 2014; 28(8):1125-36. [DOI:10.1002/ptr.5122] [PMID]
- Jafari Z, Bardania H, Barmak MJ, Eslami S, Mahmoudi-Mourderaz Y, Roustaei N, et al. Antimicrobial, anti‐inflammatory, and wound healing properties of Myrtus communis leaf methanolic extract ointment on burn wound infection induced by methicillin‐resistant staphylococcus aureus in rats. Biomed Res Int. 2024; 2024:6758817. [DOI:10.1155/2024/6758817] [PMID]
- Mahboubi M. Myrtus communis L. and its application in treatment of Recurrent Aphthous Stomatitis. J Ethnopharmacol. 2016; 193:481-9. [DOI:10.1016/j.jep.2016.09.054] [PMID]
- Harassi Y, Tilaoui M, Idir A, Frédéric J, Baudino S, Ajouaoi S, et al. Phytochemical analysis, cytotoxic and antioxidant activities of Myrtus communis essential oil from Morocco. J Complement Integr Med. 2019 Jan 19;16(3):/j/jcim.2019.16.issue-3/jcim-2018-0100/jcim-2018-0100.xml. [DOI:10.1515/jcim-2018-0100] [PMID]
- Al-Snafi AE, Teibo JO, Shaheen HM, Akinfe OA, Teibo TKA, Emieseimokumo N, et al. The therapeutic value of Myrtus communis L. : An updated review. Naunyn Schmiedebergs Arch Pharmacol. 2024; 397(7):4579-600. [DOI:10.1007/s00210-024-02958-3] [PMID]
- Kirtikar KR, Basu BD. Indian medicinal plants. Publisher not identified Basu, Bhuwaneśwari Âśrama; 1918. [DOI:10.5962/bhl.title.137025]
- Akin M, Aktumsek A, Nostro A. Antibacterial activity and composition of the essential oils of Eucalyptus camaldulensis Dehn. and Myrtus communis L. growing in Northern Cyprus. Afr J Biotechnol. 2010; 9(4). [Link]
- Hennia A, Miguel MG, Nemmiche S. Antioxidant activity of Myrtus communis L. and myrtus nivellei batt. & trab. extracts: A brief review. Medicines. 2018; 5(3):89. [DOI:10.3390/medicines5030089] [PMID]
- Mimica-Dukić N, Bugarin D, Grbović S, Mitić-Ćulafić D, Vuković-Gačić B, Orčić D, et al. Essential oil of Myrtus communis L. as a potential antioxidant and antimutagenic agents. Molecules. 2010; 15(4):2759-70. [DOI:10.3390/molecules15042759] [PMID]
- Sacchetti G, Muzzoli M, Statti G, Conforti F, Bianchi A, Agrimonti C, et al. Intra-specific biodiversity of Italian myrtle (Myrtus communis) through chemical markers profile and biological activities of leaf methanolic extracts. Nat Prod Res. 2007; 21(2):167-79. [DOI:10.1080/14786410600603783] [PMID]
- Montoro P, Tuberoso CI, Perrone A, Piacente S, Cabras P, Pizza C. Characterisation by liquid chromatography-electrospray tandem mass spectrometry of anthocyanins in extracts of Myrtus communis L. berries used for the preparation of myrtle liqueur. J Chromatogr A. 2006; 1112(1-2):232-40. [DOI:10.1016/j.chroma.2005.11.055] [PMID]
- Montoro P, Tuberoso CI, Piacente S, Perrone A, De Feo V, Cabras P, et al. Stability and antioxidant activity of polyphenols in extracts of Myrtus communis L. berries used for the preparation of myrtle liqueur. J Pharm Biomed Anal. 2006; 41(5):1614-9. [DOI:10.1016/j.jpba.2006.02.018] [PMID]
- Serce S, Ercisli S, Sengul M, Gunduz K, Orhan E. Antioxidant activities and fatty acid composition of wild grown myrtle (Myrtus communis L.) fruits. Pharmacogn Mag. 2010; 6(21):9-12. [DOI:10.4103/0973-1296.59960] [PMID]
- Sumbul S, Ahmad MA, Asif M, Saud I, Akhtar M. Evaluation of Myrtus communis Linn. berries (common myrtle) in experimental ulcer models in rats. Hum Exp Toxicol. 2010; 29(11):935-44. [DOI:10.1177/0960327110364154] [PMID]
- Romani A, Pinelli P, Mulinacci N, Vincieri FF, Tattini M. Identification and quantitation of polyphenols in leaves of Myrtus communis L. Chromatographia. 1999; 49:17-20. [DOI:10.1007/BF02467181]
- Usai M, Mulas M, Marchetti M. Chemical composition of essential oils of leaves and flowers from five cultivars of myrtle (Myrtus communis L.). J Essent Oil Res. 2015; 27(6):465-76. [DOI:10.1080/10412905.2015.1065773]
- Zomorodian K, Moein M, Lori ZG, Ghasemi Y, Rahimi MJ, Bandegani A, et al. Chemical composition and antimicrobial activities of the essential oil from Myrtus communis leaves. J Essent Oil Bearing Plants. 2013; 16(1):76-84. [DOI:10.1080/0972060X.2013.764183]
- Al-Snafi AE. Chemical constituents and pharmacological activities of Milfoil (Achillea santolina)-A Review. Int J Pharm Tech Res. 2013; 5(3):1373-7. [Link]
- Franco AM, Tocci N, Guella G, Dell’Agli M, Sangiovanni E, Perenzoni D, et al. Myrtle seeds (Myrtus communis L.) as a rich source of the bioactive ellagitannins oenothein B and eugeniflorin D2. ACS Omega. 2019; 4(14):15966-74. [DOI:10.1021/acsomega.9b02010] [PMID]
- Pedanius Dioscorides of Anazarbus. Dioscorides De Materia Medica [Beck LL, English trans]. Hildesheim: Georg Olms Verlag; 2017. [Link]
- Ghadami Yazdi E, Minaei MB, Hashem Dabaghian F, Ebrahim Zadeh Ardakani M, Ranjbar AM, Rastegari M, et al. Efficacy of Myrtus communis L. and Descurainia sophia L. versus Salicylic Acid for wart treatment. Iran Red Crescent Med J. 2014; 16(10):e16386. [PMID]
- Bagatin E, Thouvenin MD, Bacquey A, Baradat S, Lauze C, Mengeaud V, et al. The usefulness of a dermocosmetic containing Myrtus communis extract and azelaic acid for maintenance phase of adult female acne: Results from a randomized exploratory investigator‐blinded comparative study. J Eur Acad Dermatol Venereol. 2023; 37(Suppl 2):26-30. [DOI:10.1111/jdv.18795] [PMID]
- Salmanian M, Shirbeigi L, Hashem-Dabaghian F, Mansouri P, Azizkhani M, Alavi S, et al. The effects of Myrtle (Myrtus communis) and clindamycin topical solution in the treatment of mild to moderate Acne Vulgaris: A comparative split-face study. J Pharmacopuncture. 2020; 23(4):220-9. [DOI:10.3831/KPI.2020.23.4.220] [PMID]
- Mirzaee F, Jannesari S, Kariman N, Mojab F, Nasiri M. [The effect of Myrtus communis cream on wound healing and severity of episiotomy pain: Double-blind clinical trial (Persian). Iran J Obstet Gynecology Infertil. 2019; 22(8):52-61. [DOI:10.22038/ijogi.2019.13920]
- Chaijan MR, Handjani F, Zarshenas M, Rahimabadi MS, Tavakkoli A. The Myrtus communis L. solution versus ketoconazole shampoo in treatment of dandruff: A double blinded randomized clinical trial. J Pak Med Assoc. 2018; 68(5):715-20. [Link]
- Piérard-Franchimont C, Goffin V, Decroix J, Piérard GE. A multicenter randomized trial of ketoconazole 2% and zinc pyrithione 1% shampoos in severe dandruff and seborrheic dermatitis. Skin Pharmacol Appl Skin Physiol. 2002; 15(6):434-41. [DOI:10.1159/000066452] [PMID]
- Malekuti J, Mirghafourvand M, Samadi K, Abbasalizadeh F, Khodaei L. Comparison of the effect of Myrtus communis herbal and anti-hemorrhoid ointments on the hemorrhoid symptoms and quality of life in postpartum women with grade I and II internal hemorrhoid: A triple-blinded randomized controlled clinical trial. J Complement Integr Med. 2019; 16(4):20180147. [DOI:10.1515/jcim-2018-0147] [PMID]
- Zohalinezhad ME, Hosseini-Asl MK, Akrami R, Nimrouzi M, Salehi A, Zarshenas MM. Myrtus communis L. freeze-dried aqueous extract versus omeprazol in gastrointestinal reflux disease: A double-blind randomized controlled clinical trial. J Evid Based Complementary Altern Med. 2016; 21(1):23-9. [DOI:10.1177/2156587215589403] [PMID]
- Paknejad MS, Eftekhari K, Rahimi R, Vigeh M, Naghizadeh A, Karimi M. Myrtle (Myrtus communis L.) fruit syrup for gastroesophageal reflux disease in children: A double‐blind randomized clinical trial. Phytother Res. 2021; 35(11):6369-76. [DOI:10.1002/ptr.7288] [PMID]
- Rao CV, Vijayakumar M. Effect of quercetin, flavonoids and α-tocopherol, an antioxidant vitamin on experimental reflux oesophagitis in rats. Eur J Pharmacol. 2008; 589(1-3):233-8. [DOI:10.1016/j.ejphar.2008.04.062] [PMID]
- Askari SF, Jahromi BN, Dehghanian A, Zarei A, Tansaz M, Badr P, et al. Effect of a novel herbal vaginal suppository containing myrtle and oak gall in the treatment of vaginitis: a randomized clinical trial. Daru. 2020; 28(2):603-14. [DOI:10.1007/s40199-020-00365-6] [PMID]
- Masoudi M, Miraj S, Rafieian-Kopaei M. Comparison of the effects of Myrtus communis L, Berberis vulgaris and metronidazole vaginal gel alone for the treatment of bacterial vaginosis. J Clin Diagn Res. 2016; 10(3):QC04-7. [DOI:10.7860/JCDR/2016/17211.7392] [PMID]
- Qaraaty M, Kamali SH, Dabaghian FH, Zafarghandi N, Mokaberinejad R, Mobli M, et al. Effect of myrtle fruit syrup on abnormal uterine bleeding: A randomized double-blind, placebo-controlled pilot study. DARU. 2014; 22(1):45.[DOI:10.1186/2008-2231-22-45] [PMID]
- Umarami RBR, Roqaiya M, Quadri MA. Efficacy of Habbul aas (fruits of Myrtus communis) in menorrhagia: A single blinded randomized standard control study. J Complement Integr Med. 2020; 18(1):123-30. [DOI:10.1515/jcim-2018-0235] [PMID]
- Nikakhtar Z, Hasanzadeh M, Hamedi SS, Najafi MN, Tavassoli AP, Feyzabadi Z, et al. The efficacy of vaginal suppository based on myrtle in patients with cervicovaginal human papillomavirus infection: A randomized, double‐blind, placebo trial. Phytother Res. 2018; 32(10):2002-8. [DOI:10.1002/ptr.6131] [PMID]
- Khalilzadeh S, Eftkhar T, Shirbeigi L, Tabarrai M, Toliyat T, Fayazmanesh S, et al. Efficacy of a vaginal tablet as a Persian medicine product on vulvovaginal candidiasis: A double-blind, randomised, placebo-controlled trial. Pharm Biol. 2020; 58(1):574-80. [DOI:10.1080/13880209.2020.1784236] [PMID]
- Xu G, Wu M, Yang L, Liu T. [The observation and evaluation of curative effect of nasal mucosa dryness, hemorrhae and erosion (Chinese)]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021; 35(1):29-33. [PMID]
- Babaee N, Mansourian A, Momen-Heravi F, Moghadamnia A, Momen-Beitollahi J. The efficacy of a paste containing Myrtus communis (Myrtle) in the management of recurrent aphthous stomatitis: A randomized controlled trial. Clin Oral Investig. 2010; 14(1):65-70. [DOI:10.1007/s00784-009-0267-3] [PMID]
- Czakert J, Kandil FI, Boujnah H, Tavakolian P, Blakeslee SB, Stritter W, et al. Scenting serenity: Influence of essential-oil vaporization on dental anxiety-a cluster-randomized, controlled, single-blinded study (AROMA_dent). Sci Rep. 2024; 14(1):14143. [DOI:10.1038/s41598-024-63657-w] [PMID]
- D’Urso G, Montoro P, Lai C, Piacente S, Sarais G. LC-ESI/LTQOrbitrap/MS based metabolomics in analysis of Myrtus communis leaves from Sardinia (Italy). Ind Crops Prod. 2019; 128:354-62. [DOI:10.1016/j.indcrop.2018.11.022]
- Soomro S, Mesaik MA, Shaheen F, Khan N, Halim SA, Ul-Haq Z, et al. Inhibitory effects of myrtucommuacetalone 1 (MCA-1) from Myrtus Communis on inflammatory response in mouse macrophages. Molecules. 2019; 25(1):13. [DOI:10.3390/molecules25010013] [PMID]
- Cevikelli-Yakut ZA, Ertas B, Sen A, Koyuncuoglu T, Yegen BC, Sener G. Myrtus communis improves cognitive impairment in renovascular hypertensive rats. J Physiol Pharmacol. 2020; 71(5). [PMID]
- Aykac A, Ozbeyli D, Uncu M, Ertaş B, Kılınc O, Şen A, et al. Evaluation of the protective effect of Myrtus communis in scopolamine-induced Alzheimer model through cholinergic receptors. Gene. 2019; 689:194-201. [DOI:10.1016/j.gene.2018.12.007] [PMID]
- Birhanie MW, Walle B, Rebba K. Hypnotic effect of the essential oil from the leaves of Myrtus communis on mice. Nat Sci Sleep. 2016; 8:267-75. [DOI:10.2147/NSS.S101493] [PMID]
- Hajiaghaee R, Faizi M, Shahmohammadi Z, Abdollahnejad F, Naghdibadi H, Najafi F, et al. Hydroalcoholic extract of Myrtus communis can alter anxiety and sleep parameters: a behavioural and EEG sleep pattern study in mice and rats. Pharm Biol. 2016; 54(10):2141-8. [DOI:10.3109/13880209.2016.1148175] [PMID]
- Hosseinzadeh H, Khoshdel M, Ghorbani M. Antinociceptive, anti-inflammatory effects and acute toxicity of aqueous and ethanolic extracts of Myrtus communis L. Aerial parts in mice. J Acupunct Meridian Stud. 2011; 4(4):242-7. [DOI:10.1016/j.jams.2011.09.015] [PMID]
- Tumen I, Senol FS, Orhan IE. Inhibitory potential of the leaves and berries of Myrtus communis L. (myrtle) against enzymes linked to neurodegenerative diseases and their antioxidant actions. Int J Food Sci Nutr. 2012; 63(4):387-92. [DOI:10.3109/09637486.2011.629178] [PMID]
- Kadıoğlu Yaman B, Çevik Ö, Yalman K, Ertaş B, Şen A, Şener G. Myrtus communis subsp. Communis improved cognitive functions in ovariectomized diabetic rats. Gene. 2020; 744:144616. [DOI:10.1016/j.gene.2020.144616] [PMID]
- Saraiva C, Silva AC, García-Díez J, Cenci-Goga B, Grispoldi L, Silva AF, et al. Antimicrobial activity of Myrtus communis L. and Rosmarinus officinalis L. essential oils against Listeria monocytogenes in cheese. Foods. 2021; 10(5):1106. [DOI:10.3390/foods10051106] [PMID]
- Ertas B, Dorucu D, Gulerturk O, Sen A, Cevik O, Cetinel S, et al. The effect of Myrtus communis L. extract on nephrolithiasis model in rats. North Clin Istanb. 2024; 11(2):91-8. [DOI:10.14744/nci.2023.09068] [PMID]
- Coskunlu B, Koroglu MK, Hersek I, Ertas B, Sen A, Sener G, et al. Ameliorative effects of Myrtus communis L. extract involving the inhibition of oxidative stress on high fat diet-induced testis damage in rats. Biotech Histochem. 2024; 99(3):157-73. [DOI:10.1080/10520295.2024.2344491] [PMID]
- Giuliani C, Moretti RM, Bottoni M, Santagostini L, Fico G, Montagnani Marelli M. The Leaf Essential Oil of Myrtus communis subsp. tarentina (L.) Nyman: From Phytochemical Characterization to Cytotoxic and Antimigratory Activity in Human Prostate Cancer Cells. Plants. 2023; 12(6):1293. [DOI:10.3390/plants12061293] [PMID]
- Iskender B, Izgi K, Karaca H, Canatan H. Myrtucommulone-A treatment decreases pluripotency-and multipotency-associated marker expression in bladder cancer cell line HTB-9. J Nat Med. 2015; 69(4):543-54. [DOI:10.1007/s11418-015-0923-7] [PMID]
- Barhouchi B, Menacer R, Bouchkioua S, Mansour A, Belattar N. Compounds from myrtle flowers as antibacterial agents and SARS-CoV-2 inhibitors: In-vitro and molecular docking studies. Arab J Chem. 2023; 16(8):104939. [DOI:10.1016/j.arabjc.2023.104939] [PMID]
- Odeh D, Oršolić N, Berendika M, Đikić D, Domjanić Drozdek S, Balbino S, et al. Antioxidant and anti-atherogenic activities of essential oils from Myrtus communis L. and Laurus nobilis L. in rat. Nutrients. 2022; 14(7):1465. [DOI:10.3390/nu14071465] [PMID]
- Ebrahimi F, Mahmoudi J, Torbati M, Karimi P, Valizadeh H. Hemostatic activity of aqueous extract of Myrtus communis L. leaf in topical formulation: In vivo and in vitro evaluations. J Ethnopharmacol. 2020; 249:112398. [DOI:10.1016/j.jep.2019.112398] [PMID]
- Kılıç S, Okullu SÖ, Kurt Ö, Sevinç H, Dündar C, Altınordu F, et al. Efficacy of two plant extracts against acne vulgaris: Initial results of microbiological tests and cell culture studies. J Cosmet Dermatol. 2019; 18(4):1061-5. [DOI:10.1111/jocd.12814] [PMID]
- Ruffier d’Epenoux L, Fayoux E, Veziers J, Dagnelie MA, Khammari A, Dréno B, et al. Biofilm of Cutibacterium acnes: a target of different active substances. Int J Dermatol. 2024; 63(11):1541-50. [DOI:10.1111/ijd.17194] [PMID]
- Narzary I, Swarnakar A, Kalita M, Middha SK, Usha T, Babu D, et al. Acknowledging the use of botanicals to treat diabetic foot ulcer during the 21st century: A systematic review. World J Clin Cases. 2023; 11(17):4035-59. [DOI:10.12998/wjcc.v11.i17.4035] [PMID]
- Khodaie SA, Emadi F, Naseri M, Kamalinejad M, Riahi SM, Alijaniha F, et al. The Effect of Myrtus communis Aqueous Extract-Containing Gel on Wound Healing in Streptozotocin-Induced Diabetic Rats. Curr Drug Discov Technol. 2021; 18(4):542-7. [DOI:10.2174/1570163817666200712163956] [PMID]
- Ozkol H, Tuluce Y, Dilsiz N, Koyuncu I. Therapeutic potential of some plant extracts used in Turkish traditional medicine on streptozocin-induced type 1 diabetes mellitus in rats. J Membr Biol. 2013; 246(1):47-55. [DOI:10.1007/s00232-012-9503-x] [PMID]
- Ozcan O, Ipekci H, Alev B, Ustundag UV, Ak E, Sen A, et al. Protective effect of Myrtle (Myrtus communis) on burn induced skin injury. Burns. 2019; 45(8):1856-63. [DOI:10.1016/j.burns.2019.07.015] [PMID]
- Shiratake S, Nakahara T, Iwahashi H, Onodera T, Mizushina Y. Rose myrtle (Rhodomyrtus tomentosa) extract and its component, piceatannol, enhance the activity of DNA polymerase and suppress the inflammatory response elicited by UVB induced DNA damage in skin cells. Mol Med Rep. 2015; 12(4):5857-64. [DOI:10.3892/mmr.2015.4156] [PMID]
- van der Wouden JC, van der Sande R, Kruithof EJ, Sollie A, van Suijlekom-Smit LW, Koning S. Interventions for cutaneous molluscum contagiosum. Cochrane Database Syst Rev. 2017; 5(5):CD004767. [DOI:10.1002/14651858.CD004767.pub4] [PMID]
- Guzzo F, Durán AG, Sanna C, Marasco R, Molfetta N, Buommino E, et al. Gallomyrtucommulones g and h, new phloroglucinol glycosides, from bioactive fractions of Myrtus communis against Staphylococcus species. Molecules. 2022; 27(20):7109. [DOI:10.3390/molecules27207109] [PMID]
- Nourzadeh M, Amini A, Fakoor F, Raoof M, Sharififar F. Comparative antimicrobial efficacy of Eucalyptus galbie and Myrtus communis L. extracts, chlorhexidine and sodium hypochlorite against Enterococcus faecalis. Iran Endod J. 2017; 12(2):205-10.
- Jabri MA, Hajaji S, Omrani A, Ben Youssef M, Sebai H. Myrtle berries seeds prevent dyslipidemia, inflammation, and excessive cardiac reactive oxygen species production in response to high-fat diet-induced obesity. J Med Food. 2023; 26(9):631-40. [DOI:10.1089/jmf.2021.0199] [PMID]
- Sakulnarmrat K, Konczak I. Composition of native Australian herbs polyphenolic-rich fractions and in vitro inhibitory activities against key enzymes relevant to metabolic syndrome. Food Chem. 2012; 134(2):1011-9. [DOI:10.1016/j.foodchem.2012.02.217] [PMID]
- Saadat S, Beigoli S, Khazdair MR, Amin F, Boskabady MH. Experimental and clinical studies on the effects of natural products on noxious agents-induced lung disorders, a review. Front Nutr. 2022; 9:867914. [DOI:10.3389/fnut.2022.867914] [PMID]
- Rapiejko P, Talik P, Jurkiewicz D. New treatment options for acute rhinosinusitis according to EPOS 2020. Otolaryngol Pol. 2021; 76(1):29-39. [DOI:10.5604/01.3001.0015.7094] [PMID]
- Alam MA, Quamri MA, Sofi G, Ayman U, Ansari S, Ahad M. Understanding COVID-19 in the light of epidemic disease described in Unani medicine. Drug Metab Pers Ther. 2020; 35(4). [DOI:10.1515/dmpt-2020-0136] [PMID]
- Mehrbod P, Safari H, Mollai Z, Fotouhi F, Mirfakhraei Y, Entezari H, et al. Potential antiviral effects of some native Iranian medicinal plants extracts and fractions against influenza A virus. BMC Complement Med Ther. 2021; 21(1):246. [DOI:10.1186/s12906-021-03423-x] [PMID]
- Hua H, Li F, Xi Y, Jiao W, Wen S, Tao Z. [To explore the therapeutic effect of myrtle oil, anthocyanin and hyaluronic acid in combination with topical application on allergic rhinitis in rats exposed to PM2.5 (Chinese)]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020; 34(8):719-25. [PMID]
- Prall S, Bowles EJ, Bennett K, Cooke CG, Agnew T, Steel A, et al. Effects of essential oils on symptoms and course (duration and severity) of viral respiratory infections in humans: A rapid review. Adv Integr Med. 2020; 7(4):218-21. [DOI:10.1016/j.aimed.2020.07.005] [PMID]
- Rajizadeh MA, Najafipour H, Samareh Fekr M, Rostamzadeh F, Jafari E, Bejeshk MA, et al. Anti-Inflammatory and Anti-Oxidative Effects of Myrtenol in the Rats with Allergic Asthma. Iran J Pharm Res. 2019; 18(3):1488-98. [PMID]
- Samareh Fekri M, Mandegary A, Sharififar F, Poursalehi HR, Nematollahi MH, Izadi A, et al. Protective effect of standardized extract of Myrtus communis L. (myrtle) on experimentally bleomycin-induced pulmonary fibrosis: Biochemical and histopathological study. Drug Chem Toxicol. 2018; 41(4):408-14. [DOI:10.1080/01480545.2018.1459670] [PMID]
- Khadraoui N, Essid R, Damergi B, Fares N, Gharbi D, Forero AM, et al. Myrtus communis leaf compounds as novel inhibitors of quorum sensing-regulated virulence factors and biofilm formation: In vitro and in silico investigations. Biofilm. 2024; 8:100205. [DOI:10.1016/j.bioflm.2024.100205] [PMID]
- Kabatas GS, Ertas B, Sen A, Sener G, Ercan F, Akakin D. Histological and biochemical effects of an ethanolic extract of Myrtus communis leaf on the pancreases of rats fed high fat diets. Biotech Histochem. 2024; 99(4):204-15. [DOI:10.1080/10520295.2024.2355212] [PMID]
- Knauthe A, Mittag S, Bloch L, Albring KF, Schmidt M, Werz O, et al. Hyperforin and myrtucommulone derivatives act as natural modulators of Wnt/β-catenin signaling in HCT116 colon cancer cells. Int J Mol Sci. 2022; 23(6):2984. [DOI:10.3390/ijms23062984] [PMID]
- Mansour RB, Beji RS, Wasli H, Zekri S, Ksouri R, Megdiche-Ksouri W, et al. Gastroprotective effect of microencapsulated Myrtus communis essential oil against ethanol/HCl-induced acute gastric lesions. Molecules. 2022; 27(5):1566. [DOI:10.3390/molecules27051566] [PMID]
- Jabri MA, Hajaji S, Rtibi K, Sebai H. Role of anti-inflammatory, reactive oxygen species scavenging activity and nematicidal properties of Myrtle berry seeds on Helminthiasis treatment. J Med Food. 2021; 24(4):377-84. [DOI:10.1089/jmf.2020.0089] [PMID]
- Mahmoudvand H, Fallahi S, Mahmoudvand H, Shakibaie M, Harandi MF, Dezaki ES. Efficacy of Myrtus communis L. to inactivate the hydatid cyst protoscoleces. J Invest Surg. 2016; 29(3):137-43. [DOI:10.3109/08941939.2015.1088601] [PMID]
- Hedayati A, Khosropanah H, Bazargani A, Abed M, Emami A. Assessing the antimicrobial effect of the essential oil of Myrtus communis on the clinical isolates of Porphyromonas gingivalis: An in vitro study. Jundishapur J Nat Pharm Prod. 2013; 8(4):165-8. [DOI:10.17795/jjnpp-12253] [PMID]
- Sateriale D, Facchiano S, Colicchio R, Pagliuca C, Varricchio E, Paolucci M, et al. In vitro synergy of polyphenolic extracts from honey, myrtle and pomegranate against oral pathogens, S. mutans and R. dentocariosa. Front Microbiol. 2020; 11:1465. [DOI:10.3389/fmicb.2020.01465] [PMID]
- Torabi I, Sharififar F, Izadi A, Ayatollahi Mousavi SA. Inhibitory effects of different fractions separated from standardized extract of Myrtus communis L. against nystatin-susceptible and nystatin-resistant Candida albicans isolated from HIV positive patients. Heliyon. 2022; 8(3):e09073. [DOI:10.1016/j.heliyon.2022.e09073] [PMID]
- Hassan HA, El-Kholy WM, El-Sawi MR, Galal NA, Ramadan MF. Myrtle (Myrtus communis) leaf extract suppresses hepatotoxicity induced by monosodium glutamate and acrylamide through obstructing apoptosis, DNA fragmentation, and cell cycle arrest. Environ Sci Pollut Res Int. 2020; 27(18):23188-98. [DOI:10.1007/s11356-020-08780-7] [PMID]
- Ben Hsouna A, Dhibi S, Dhifi W, Mnif W, Ben Nasr H, Hfaiedh N. Chemical composition and hepatoprotective effect of essential oil from Myrtus communis L. flowers against CCL 4-induced acute hepatotoxicity in rats. RSC Adv. 2019; 9(7):3777-87. [DOI:10.1039/C8RA08204A] [PMID]
- Ozbeyli D, Sen A, Cilingir Kaya OT, Ertas B, Aydemir S, Ozkan N, et al. Myrtus communis leaf extract protects against cerulein‐induced acute pancreatitis in rats.J Food Biochem. 2020; 44(2):e13130. [DOI:10.1111/jfbc.13130] [PMID]
- Hashemipour MA, Lotfi S, Torabi M, Sharifi F, Ansari M, Ghassemi A, et al. Evaluation of the effects of three plant Species (Myrtus Communis L., Camellia Sinensis L., Zataria Multiflora Boiss.) on the Healing Process of Intraoral Ulcers in Rats. J Dent (Shiraz). 2017; 18(2):127-35. [PMID]
- Jabri MA, Rtibi K, Sakly M, Marzouki L, Sebai H. Role of gastrointestinal motility inhibition and antioxidant properties of myrtle berries (Myrtus communis L.) juice in diarrhea treatment. Biomed Pharmacother. 2016; 84:1937-44. [DOI:10.1016/j.biopha.2016.11.008] [PMID]
- Sisay M, Engidawork E, Shibeshi W. Evaluation of the antidiarrheal activity of the leaf extracts of Myrtus communis Linn (Myrtaceae) in mice model. BMC Complement Altern Med. 2017; 17(1):103. [DOI:10.1186/s12906-017-1625-3] [PMID]
- Sen A, Ozkan S, Recebova K, Cevik O, Ercan F, Kervancıoglu Demirci E, et al. Effects of Myrtus communis extract treatment in bile duct ligated rats. J Surg Res. 2016; 205(2):359-67. [DOI:10.1016/j.jss.2016.06.094] [PMID]
- Deriu A, Branca G, Molicotti P, Pintore G, Chessa M, Tirillini B, et al. In vitro activity of essential oil of Myrtus communis L. against Helicobacter pylori. Int J Antimicrob Agents. 2007; 30(6):562-3. [DOI:10.1016/j.ijantimicag.2007.07.005] [PMID]
- Zaidi SF, Muhammad JS, Shahryar S, Usmanghani K, Gilani AH, Jafri W, et al. Anti-inflammatory and cytoprotective effects of selected Pakistani medicinal plants in Helicobacter pylori-infected gastric epithelial cells. J Ethnopharmacol. 2012; 141(1):403-10. [DOI:10.1016/j.jep.2012.03.001] [PMID]
- Belahcene S, Kebsa W, Omoboyowa DA, Alshihri AA, Alelyani M, Bakkour Y, et al. Unveiling the chemical profiling antioxidant and anti-inflammatory activities of algerian myrtus communis l. essential oils, and exploring molecular docking to predict the inhibitory compounds against cyclooxygenase-2. Pharmaceuticals. 2023; 16(10):1343. [DOI:10.3390/ph16101343] [PMID]
- Amira S, Dade M, Schinella G, Ríos JL. Anti-inflammatory, anti-oxidant, and apoptotic activities of four plant species used in folk medicine in the Mediterranean basin. Pak J Pharm Sci. 2012; 25(1):65-72. [PMID]
- Belahcene S, Kebsa W, Akingbade TV, Umar HI, Omoboyowa DA, Alshihri AA, et al. Chemical composition antioxidant and anti-inflammatory activities of Myrtus communis L. leaf extract: forecasting ADMEt profiling and anti-inflammatory targets using molecular docking tools. Molecules. 2024; 29(4):849. [DOI:10.3390/molecules29040849] [PMID]
- Maxia A, Frau MA, Falconieri D, Karchuli MS, Kasture S. Essential oil of Myrtus communis inhibits inflammation in rats by reducing serum IL-6 and TNF-α. Nat Prod Commun. 2011; 6(10):1934578X1100601034. [DOI:10.1177/1934578X1100601034]
- Mir MA, Bashir N, Alfaify A, Oteef MDY. GC-MS analysis of Myrtus communis extract and its antibacterial activity against gram-positive bacteria. BMC Complement Med Ther. 2020; 20(1):86. [DOI:10.1186/s12906-020-2863-3] [PMID]
- Hayani M, Benabbouha T, Naceiri Mrabti N, Eljebri S, Sabiri M, Zair T. Bioactive profiling, antibacterial efficacy and computational modelling of Myrtus communis essential oil (Morocco). Chem Biodivers. 2024; 21(6):e202302114.[DOI:10.1002/cbdv.202302114] [PMID]
- Polat Yemiş G, Sezer E, Sıçramaz H. Inhibitory effect of sodium alginate nanoemulsion coating containing myrtle essential oil (Myrtus communis L.) on listeria monocytogenes in Kasar Cheese. Molecules. 2022; 27(21):7298. [DOI:10.3390/molecules27217298] [PMID]
- Fadil M, Fikri-Benbrahim K, Rachiq S, Ihssane B, Lebrazi S, Chraibi M, et al. Combined treatment of Thymus vulgaris L., Rosmarinus officinalis L. and Myrtus communis L. essential oils against Salmonella typhimurium: Optimization of antibacterial activity by mixture design methodology. Eur J Pharm Biopharm. 2018; 126:211-20. [DOI:10.1016/j.ejpb.2017.06.002] [PMID]
- Hesami D, Ghaffarifar F, Dalimi A, Dayer MS, Nasiri V, Sheikh S. Investigating in vivo and in vitro effects of ethanolic and aqueous extracts of Myrtle (Myrtus communis) on Leishmania major. Iran J Parasitol. 2021; 16(4):641-51. [DOI:10.18502/ijpa.v16i4.7877] [PMID]
- Et-Tazy L, Lamiri A, Satia L, Essahli M, Krimi Bencheqroun S. In vitro antioxidant and antifungal activities of four essential oils and their major compounds against post-harvest fungi associated with chickpea in storage. Plants. 2023; 12(20):3587. [DOI:10.3390/plants12203587] [PMID]
Type of Study: Review article |
Subject:
Medicine and traditional medicine
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
