

Volume 11, Issue 3 (2025)
Pharm Biomed Res 2025, 11(3): 271-276 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseini S H, Ghazvini H, Tamijani S M S, Rafaiee R. Urinary Incontinence During Sleep Associated With Buspirone: A Case Report. Pharm Biomed Res 2025; 11 (3) :271-276
URL: http://pbr.mazums.ac.ir/article-1-693-en.html
URL: http://pbr.mazums.ac.ir/article-1-693-en.html
Seyed Hamzeh Hosseini1 

 , Hamed Ghazvini2 , Seyedeh Masoumeh Seyedhosseini Tamijani2 , Raheleh Rafaiee *3
, Hamed Ghazvini2 , Seyedeh Masoumeh Seyedhosseini Tamijani2 , Raheleh Rafaiee *3
, Hamed Ghazvini2 , Seyedeh Masoumeh Seyedhosseini Tamijani2 , Raheleh Rafaiee *3
1- Department of Psychiatry, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Neuroscience, Faculty of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Neuroscience, Faculty of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran. & Psychiatry and Behavioral Sciences Research Center, Addiction Research Institute, Mazandaran University of Medical Sciences, Sari, Iran.
2- Department of Neuroscience, Faculty of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
3- Department of Neuroscience, Faculty of Advanced Technologies in Medicine, Mazandaran University of Medical Sciences, Sari, Iran. & Psychiatry and Behavioral Sciences Research Center, Addiction Research Institute, Mazandaran University of Medical Sciences, Sari, Iran.
Full-Text [PDF 510 kb]
(684 Downloads)
| Abstract (HTML) (871 Views)
Full-Text: (376 Views)
Introduction
Buspirone is an anxiolytic medication with a unique pharmacological profile that distinguishes it from traditional benzodiazepines. Buspirone is categorized as “anxioselective,” meaning it selectively alleviates anxiety without the anticonvulsant, sedative, or muscle-relaxant effects associated with benzodiazepines [1]. It has been shown to lack the potential for abuse and physical dependence, distinguishing it from traditional anxiolytics [2]. Buspirone acts as a partial agonist at serotonin 5-HT1A receptors and exhibits both agonist and antagonist properties at dopamine receptors [3]. Buspirone enhances dopaminergic activity by inhibiting dopamine autoreceptors, possibly contributing to its anxiolytic effect [4]. Buspirone does not interact with the benzodiazepine receptor complex, differentiating its action from benzodiazepines [5].
Although buspirone is effective in treating anxiety, it is associated with several side effects that warrant consideration. Some patients who used buspirone reported drowsiness, weakness, and faintness, particularly at higher doses (20 mg) [6]. Also, animal studies have indicated potential amnesic effects of high doses of buspirone, impairing performance in tasks related to memory and learning [7]. Buspirone increases sleep latency and decreases total sleep duration, affecting both non-rapid eye movement (non-REM) and rapid eye movement (REM) sleep [8]. Unlike many anxiolytics, buspirone does not exhibit significant sedative properties, making it a preferable option for those concerned about daytime alertness [9].
The effects of buspirone on sleep may indirectly influence urinary patterns, as it has been shown to disrupt sleep stages without sedative effects [10]. This disruption could exacerbate nocturnal incontinence. To our knowledge, no cases of buspirone-induced urinary incontinence have been reported. According to the medical literature, urinary incontinence is listed as infrequent adverse effect of buspirone, occurring in less than 1% of patients; however, detailed case reports describing this association are lacking [11, 12]. In the present study, we discuss the case of a 52-year-old woman who had been treated for depression for more than 26 years. She developed urinary incontinence during sleep after prescribing buspirone.
Case Presentation
We report a 52-year-old married female patient who was admitted to the Psychiatric Clinic with nocturnal enuresis 2 months ago. The patient has been suffering from depression for 26 years. At the time of referral to our clinic, the patient was undergoing antidepressant therapy but reported a gradual decline in mood stability over the preceding weeks, accompanied by reduced motivation, low energy, and diminished pleasure in daily routines. She also described a mild sleep quality and appetite deterioration, though without significant weight change. Her psychiatric history spanned more than two decades, during which several psychiatrists had treated her; however, detailed recollections of her initial symptom profile were limited due to the chronicity of her illness. Given the persistence of these residual depressive symptoms despite stable pharmacotherapy, buspirone 10 mg/day was initiated as an augmentation measure.
She had no history of chronic diseases such as thyroid disease, respiratory disease, hypertension, or diabetes. She had no history of drug or food allergies, urinary tract infection, kidney disease, pelvic surgery, or childhood enuresis. Physical examination findings were normal, and the rest of the clinical examination, including the gynecologic and neurologic examination, revealed no significant findings.
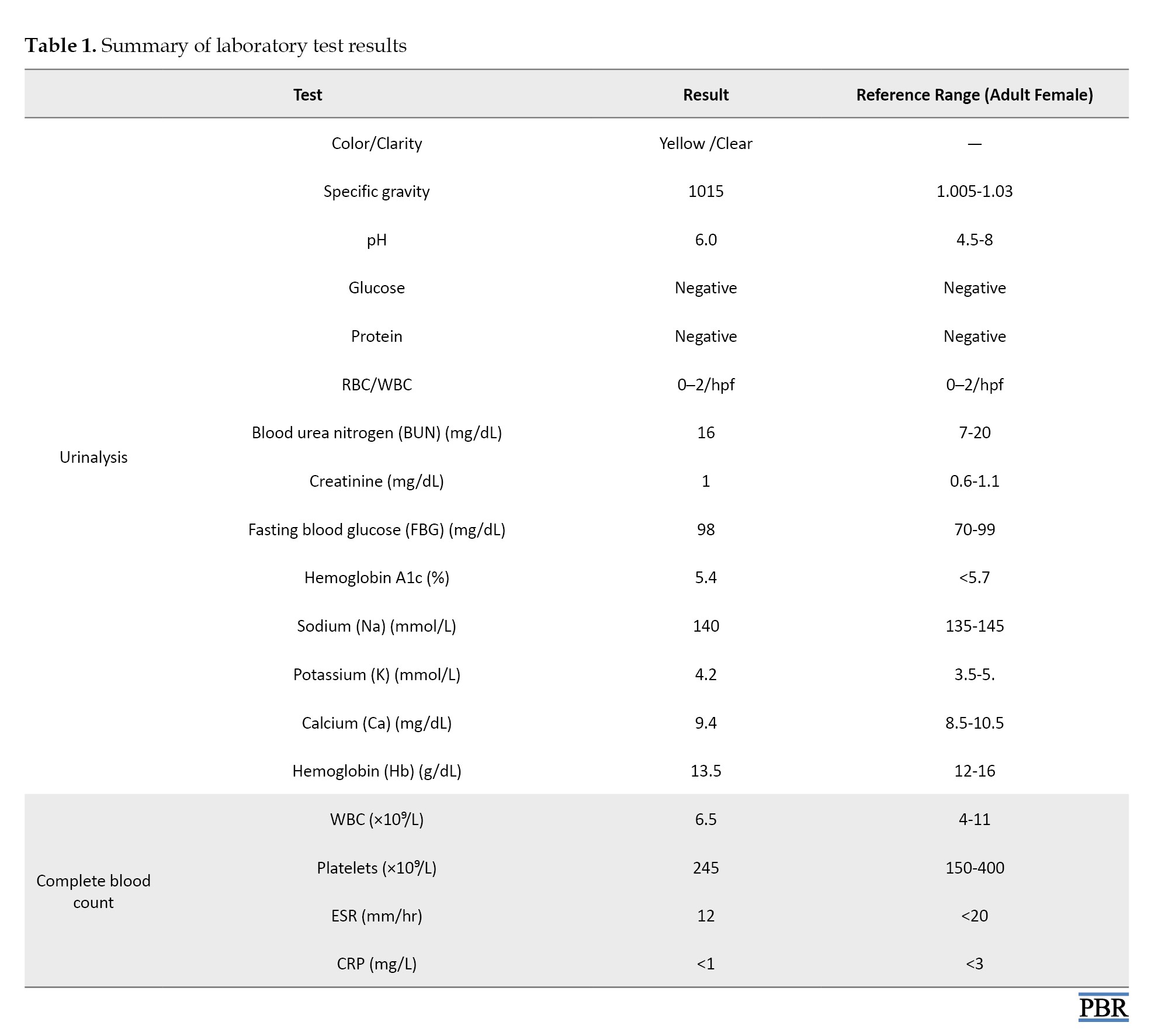
Laboratory evaluations, urinalysis, and renal function tests yielded results within normal limits, effectively excluding urinary tract infection, renal dysfunction, and metabolic disorders. Table 1 presents a summary of the laboratory tests.
At the time of presentation, the patient had a longstanding diagnosis of major depressive disorder in partial remission. She had been maintained for several months on a stable regimen of fluoxetine 10 mg twice daily (total daily dose 20 mg) and pregabalin 100 mg twice daily (total daily dose 200 mg). Approximately two months prior to the onset of symptoms, buspirone 10 mg/day was added (not for the treatment of anxiety symptoms), as part of a structured “step 2” augmentation strategy for partial response to antidepressant therapy, consistent with the approach evaluated in the sequenced treatment alternatives to relieve depression (STAR*D) trial. In that trial, buspirone, acting as a partial agonist at 5HT1A receptors, was one of the recommended augmentation options to enhance selective serotonin reuptake inhibitor (SSRI) efficacy in patients with incomplete remission after initial monotherapy [13].
Approximately one week after starting buspirone, the patient developed nocturnal enuresis, occurring once or twice a week. This led her husband to sleep in a separate bed, causing significant embarrassment and emotional distress. She tolerated the situation for approximately one month without suspecting a potential link to the new medication. There were no daytime urinary symptoms, dysuria, hematuria, fever, pelvic pain, neurological deficits, or changes in bowel or fluid intake. At a subsequent psychiatric followup visit, she reported the problem, and buspirone was discontinued. No alternative augmentation agent was initiated, and her maintenance regimen of fluoxetine and pregabalin was continued.
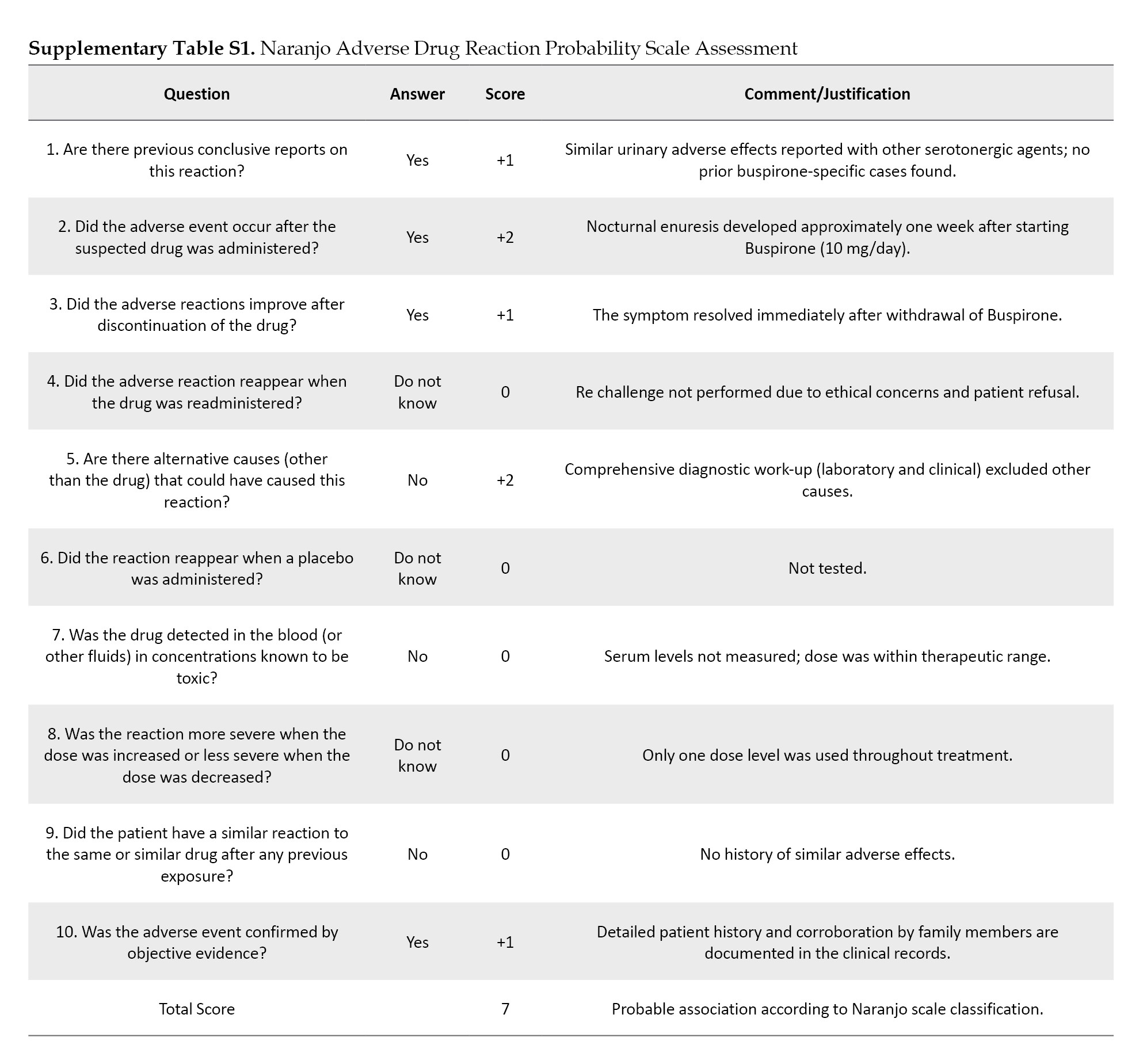
The patient’s nocturnal enuresis disappeared immediately after the discontinuation of buspirone. Over the ensuing six months, the nocturnal enuresis did not recur. Causality assessment using the Naranjo adverse drug reaction probability scale produced a total score of 7, indicating a probable association; detailed scoring is provided in Supplementary Table S1.
Discussion
We present a case of nocturnal enuresis associated with buspirone. To the best of our knowledge, case reports of nocturnal urinary incontinence in buspirone users have not been published. Although medical literature reports [11, 12] urinary incontinence as a rare adverse effect (<1%) of buspirone, our report provides detailed clinical observations and a clear temporal relationship supporting this association. Causality assessment using the Naranjo algorithm yielded a score of 7, indicating a probable relationship. Rechallenge was not performed due to ethical considerations and the patient’s refusal.
Studies have indicated that the use of SSRIs is associated with a 61% increased risk of urinary incontinence, particularly in the elderly [14]. The incidence density ratio for urinary incontinence during SSRI exposure is notably high, with sertraline users facing even greater risk [14].
Individual patient characteristics and medical history can influence the incidence of nocturnal urinary incontinence as a side effect of antidepressants. The medical literature indicates that genetic factors, comorbid conditions, and demographic variables significantly predicts nocturnal urinary incontinence [15, 16]. Studies show that the female gender is associated with a higher incidence of urinary incontinence when treated with certain medications [17]. Age-related factors also contribute; elderly patients often experience higher rates of urinary incontinence due to a combination of medication effects and age-related physiological changes [18].
Antidepressants, particularly serotonin and norepinephrine reuptake inhibitors, such as duloxetine, can lead to nocturnal urinary incontinence through several neurophysiological mechanisms. These medications influence neurotransmitter systems that modulate bladder control, altering micturition patterns. Duloxetine enhances the activity of pudendal motor neurons, increasing urethral sphincter contractility, which can paradoxically lead to incontinence in some patients [19, 20]. Also, antidepressants affect central nervous system pathways that regulate bladder function, potentially decreasing inhibitory control and increasing detrusor muscle sensitivity [21, 22].
The use of serotonergic antidepressants has been linked to conditions like REM sleep behavior disorder, which may indirectly affect nocturnal urinary control. Adverse effects such as the syndrome of inappropriate antidiuretic hormone are more prevalent with serotonergic agents, potentially leading to increased nocturnal urination [23].
We hypothesize that buspirone-induced modulation of serotonergic and dopaminergic neurotransmission may impair micturition control during sleep. Specifically, partial agonism at presynaptic and postsynaptic 5HT1A receptors may decrease inhibitory serotonergic tone on the pontine micturition center, leading to increased detrusor activity. Dopaminergic effects may further influence bladder reflexes. Moreover, buspirone’s documented alterations in sleep architecture could diminish arousal thresholds, preventing awakening before bladder emptying. These factors can synergistically promote nocturnal urinary incontinence in predisposed patients.
While these medications can alleviate anxiety and improve quality of life, they may also influence urinary function, especially in individuals with serotonergic dysregulation. Reporting rare drug side effects is crucial for enhancing patient safety and improving pharmacovigilance. The lessons learned from case reports highlight the importance of effective monitoring, and data analysis in understanding the adverse effects of medications.
Ethical Considerations
Compliance with ethical guidelines
This study was designed based on the ethical principles of the Declaration of Helsinki (2008) for medical studies involving humans. This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1403.260). Informed consent was obtained from the patient before publication.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design and project administration: Seyed Hamzeh Hosseini; Data collection: Raheleh Rafaiee; Data interpretation: Hamed Ghazvini, and Seyedeh Masoumeh Seyedhosseini Tamijani; Writing: Raheleh Rafaiee; Hamed Ghazvini, and Seyedeh Masoumeh Seyedhosseini Tamijani; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patient in this study. Moreover, they thank Mazandaran University of Medical Sciences, Sari, Iran.
References
Buspirone is an anxiolytic medication with a unique pharmacological profile that distinguishes it from traditional benzodiazepines. Buspirone is categorized as “anxioselective,” meaning it selectively alleviates anxiety without the anticonvulsant, sedative, or muscle-relaxant effects associated with benzodiazepines [1]. It has been shown to lack the potential for abuse and physical dependence, distinguishing it from traditional anxiolytics [2]. Buspirone acts as a partial agonist at serotonin 5-HT1A receptors and exhibits both agonist and antagonist properties at dopamine receptors [3]. Buspirone enhances dopaminergic activity by inhibiting dopamine autoreceptors, possibly contributing to its anxiolytic effect [4]. Buspirone does not interact with the benzodiazepine receptor complex, differentiating its action from benzodiazepines [5].
Although buspirone is effective in treating anxiety, it is associated with several side effects that warrant consideration. Some patients who used buspirone reported drowsiness, weakness, and faintness, particularly at higher doses (20 mg) [6]. Also, animal studies have indicated potential amnesic effects of high doses of buspirone, impairing performance in tasks related to memory and learning [7]. Buspirone increases sleep latency and decreases total sleep duration, affecting both non-rapid eye movement (non-REM) and rapid eye movement (REM) sleep [8]. Unlike many anxiolytics, buspirone does not exhibit significant sedative properties, making it a preferable option for those concerned about daytime alertness [9].
The effects of buspirone on sleep may indirectly influence urinary patterns, as it has been shown to disrupt sleep stages without sedative effects [10]. This disruption could exacerbate nocturnal incontinence. To our knowledge, no cases of buspirone-induced urinary incontinence have been reported. According to the medical literature, urinary incontinence is listed as infrequent adverse effect of buspirone, occurring in less than 1% of patients; however, detailed case reports describing this association are lacking [11, 12]. In the present study, we discuss the case of a 52-year-old woman who had been treated for depression for more than 26 years. She developed urinary incontinence during sleep after prescribing buspirone.
Case Presentation
We report a 52-year-old married female patient who was admitted to the Psychiatric Clinic with nocturnal enuresis 2 months ago. The patient has been suffering from depression for 26 years. At the time of referral to our clinic, the patient was undergoing antidepressant therapy but reported a gradual decline in mood stability over the preceding weeks, accompanied by reduced motivation, low energy, and diminished pleasure in daily routines. She also described a mild sleep quality and appetite deterioration, though without significant weight change. Her psychiatric history spanned more than two decades, during which several psychiatrists had treated her; however, detailed recollections of her initial symptom profile were limited due to the chronicity of her illness. Given the persistence of these residual depressive symptoms despite stable pharmacotherapy, buspirone 10 mg/day was initiated as an augmentation measure.
She had no history of chronic diseases such as thyroid disease, respiratory disease, hypertension, or diabetes. She had no history of drug or food allergies, urinary tract infection, kidney disease, pelvic surgery, or childhood enuresis. Physical examination findings were normal, and the rest of the clinical examination, including the gynecologic and neurologic examination, revealed no significant findings.
Laboratory evaluations, urinalysis, and renal function tests yielded results within normal limits, effectively excluding urinary tract infection, renal dysfunction, and metabolic disorders. Table 1 presents a summary of the laboratory tests.
At the time of presentation, the patient had a longstanding diagnosis of major depressive disorder in partial remission. She had been maintained for several months on a stable regimen of fluoxetine 10 mg twice daily (total daily dose 20 mg) and pregabalin 100 mg twice daily (total daily dose 200 mg). Approximately two months prior to the onset of symptoms, buspirone 10 mg/day was added (not for the treatment of anxiety symptoms), as part of a structured “step 2” augmentation strategy for partial response to antidepressant therapy, consistent with the approach evaluated in the sequenced treatment alternatives to relieve depression (STAR*D) trial. In that trial, buspirone, acting as a partial agonist at 5HT1A receptors, was one of the recommended augmentation options to enhance selective serotonin reuptake inhibitor (SSRI) efficacy in patients with incomplete remission after initial monotherapy [13].
Approximately one week after starting buspirone, the patient developed nocturnal enuresis, occurring once or twice a week. This led her husband to sleep in a separate bed, causing significant embarrassment and emotional distress. She tolerated the situation for approximately one month without suspecting a potential link to the new medication. There were no daytime urinary symptoms, dysuria, hematuria, fever, pelvic pain, neurological deficits, or changes in bowel or fluid intake. At a subsequent psychiatric followup visit, she reported the problem, and buspirone was discontinued. No alternative augmentation agent was initiated, and her maintenance regimen of fluoxetine and pregabalin was continued.
The patient’s nocturnal enuresis disappeared immediately after the discontinuation of buspirone. Over the ensuing six months, the nocturnal enuresis did not recur. Causality assessment using the Naranjo adverse drug reaction probability scale produced a total score of 7, indicating a probable association; detailed scoring is provided in Supplementary Table S1.
Discussion
We present a case of nocturnal enuresis associated with buspirone. To the best of our knowledge, case reports of nocturnal urinary incontinence in buspirone users have not been published. Although medical literature reports [11, 12] urinary incontinence as a rare adverse effect (<1%) of buspirone, our report provides detailed clinical observations and a clear temporal relationship supporting this association. Causality assessment using the Naranjo algorithm yielded a score of 7, indicating a probable relationship. Rechallenge was not performed due to ethical considerations and the patient’s refusal.
Studies have indicated that the use of SSRIs is associated with a 61% increased risk of urinary incontinence, particularly in the elderly [14]. The incidence density ratio for urinary incontinence during SSRI exposure is notably high, with sertraline users facing even greater risk [14].
Individual patient characteristics and medical history can influence the incidence of nocturnal urinary incontinence as a side effect of antidepressants. The medical literature indicates that genetic factors, comorbid conditions, and demographic variables significantly predicts nocturnal urinary incontinence [15, 16]. Studies show that the female gender is associated with a higher incidence of urinary incontinence when treated with certain medications [17]. Age-related factors also contribute; elderly patients often experience higher rates of urinary incontinence due to a combination of medication effects and age-related physiological changes [18].
Antidepressants, particularly serotonin and norepinephrine reuptake inhibitors, such as duloxetine, can lead to nocturnal urinary incontinence through several neurophysiological mechanisms. These medications influence neurotransmitter systems that modulate bladder control, altering micturition patterns. Duloxetine enhances the activity of pudendal motor neurons, increasing urethral sphincter contractility, which can paradoxically lead to incontinence in some patients [19, 20]. Also, antidepressants affect central nervous system pathways that regulate bladder function, potentially decreasing inhibitory control and increasing detrusor muscle sensitivity [21, 22].
The use of serotonergic antidepressants has been linked to conditions like REM sleep behavior disorder, which may indirectly affect nocturnal urinary control. Adverse effects such as the syndrome of inappropriate antidiuretic hormone are more prevalent with serotonergic agents, potentially leading to increased nocturnal urination [23].
We hypothesize that buspirone-induced modulation of serotonergic and dopaminergic neurotransmission may impair micturition control during sleep. Specifically, partial agonism at presynaptic and postsynaptic 5HT1A receptors may decrease inhibitory serotonergic tone on the pontine micturition center, leading to increased detrusor activity. Dopaminergic effects may further influence bladder reflexes. Moreover, buspirone’s documented alterations in sleep architecture could diminish arousal thresholds, preventing awakening before bladder emptying. These factors can synergistically promote nocturnal urinary incontinence in predisposed patients.
While these medications can alleviate anxiety and improve quality of life, they may also influence urinary function, especially in individuals with serotonergic dysregulation. Reporting rare drug side effects is crucial for enhancing patient safety and improving pharmacovigilance. The lessons learned from case reports highlight the importance of effective monitoring, and data analysis in understanding the adverse effects of medications.
Ethical Considerations
Compliance with ethical guidelines
This study was designed based on the ethical principles of the Declaration of Helsinki (2008) for medical studies involving humans. This study was approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (Code: IR.MAZUMS.REC.1403.260). Informed consent was obtained from the patient before publication.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design and project administration: Seyed Hamzeh Hosseini; Data collection: Raheleh Rafaiee; Data interpretation: Hamed Ghazvini, and Seyedeh Masoumeh Seyedhosseini Tamijani; Writing: Raheleh Rafaiee; Hamed Ghazvini, and Seyedeh Masoumeh Seyedhosseini Tamijani; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the patient in this study. Moreover, they thank Mazandaran University of Medical Sciences, Sari, Iran.
References
- Basile AS, Lippa AS, Skolnick P. Anxioselective anxiolytics: Can less be more? Eur J Pharmacol. 2004; 500(1-3):441-51. [DOI:10.1016/j.ejphar.2004.07.043] [PMID]
- Gunter BW. Evaluation of the anxiolytic-like, abuse-related, and sedative/motor effects of benzodiazepine and neuroactive steroid combinations in rats [PhD dissertation]. Mississippi: University of Mississippi Medical Center; 2015. [Link]
- Smith ALW, Harmer CJ, Cowen PJ, Murphy SE. The Serotonin 1A (5-HT1A) receptor as a pharmacological target in depression. CNS Drugs. 2023; 37(7):571-85. [DOI:10.1007/s40263-023-01014-7] [PMID]
- Dhavalshankh AG, Dhavalshankh GP. Psychopharmacological Profile of Buspirone: A critical overview. J Pharm Res. 2012; 5(8):3973-80. [Link]
- Loane C, Politis M. Buspirone: What is it all about? Brain Res. 2012; 1461:111-8. [DOI:10.1016/j.brainres.2012.04.032] [PMID]
- Shenoi SD, Soman S, Munoli R, Prabhu S. Update on pharmacotherapy in psychodermatological disorders. Indian Dermatol Online J. 2020; 11(3):307-18. [DOI:10.4103/idoj.IDOJ_330_19] [PMID]
- Haleem DJ, Nawaz S, Salman T. Dose related effects of buspirone on pain, learning / memory and food intake. Regul Toxicol Pharmacol. 2018; 99:182-90. [DOI:10.1016/j.yrtph.2018.09.017] [PMID]
- Hutka P, Krivosova M, Muchova Z, Tonhajzerova I, Hamrakova A, Mlyncekova Z, et al. Association of sleep architecture and physiology with depressive disorder and antidepressants treatment. Int J Mol Sci. 2021; 22(3):1333. [DOI:10.3390/ijms22031333] [PMID]
- Misra AK, Sharma PK. Sedative and hypnotic drugs. In: Uddin S, Rashid M, editor. Advances in neuropharmacology: Drugs and therapeutics. Massachusetts: Apple Academic Press; 2020. [DOI:10.1201/9780429242717-13]
- Barnett SR, Riddle MA. Anxiolytics and sedative/hypnotics: Benzodiazepines, buspirone, and others. In: Martin A, Scahill L, Kratochvil Ch, editors. Pediatric psychopharmacology. Oxford: Oxford Academic; 2010. [DOI:10.1093/med/9780195398212.003.0024]
- Drugs.com. Buspirone Side effects [Internet]. 2025 [Updated 22 May 2025]. Available from: [Link]
- Medscape. buspirone (Rx) [Internet[. New York: Medscape; 2025. [Link]
- Trivedi MH, Fava M, Wisniewski SR, Thase ME, Quitkin F, Warden D, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med. 2006; 354(12):1243-52 [DOI:10.1056/NEJMoa052964] [PMID]
- Movig KL, Leufkens HG, Belitser SV, Lenderink AW, Egberts AC. Selective serotonin reuptake inhibitor‐induced urinary incontinence. Pharmacoepidemiol Drug Saf. 2002; 11(4):271-9. [DOI:10.1002/pds.705] [PMID]
- Breinbjerg A, Jørgensen CS, Borg B, Rittig S, Kamperis K, Christensen JH. The genetics of incontinence: A scoping review. Clin Genet. 2023; 104(1):22-62. [DOI:10.1111/cge.14331] [PMID]
- Coyne KS, Kaplan SA, Chapple CR, Sexton CC, Kopp ZS, Bush EN, et al. Risk factors and comorbid conditions associated with lower urinary tract symptoms: EpiLUTS. BJU Int. 2009; 103(Suppl 3):24-32. [DOI:10.1111/j.1464-410X.2009.08438.x] [PMID]
- Tsakiris P, Oelke M, Michel MC. Drug-induced urinary incontinence. Drugs Aging. 2008; 25(7):541-9. [DOI:10.2165/00002512-200825070-00001] [PMID]
- Shaw C, Wagg A. Urinary incontinence in older adults. Medicine. 2017; 45(1):23-7. [DOI:10.1016/j.mpmed.2016.10.001]
- Noël S, Claeys S, Hamaide A. Acquired urinary incontinence in the bitch: update and perspectives from human medicine. Part 2: The urethral component, pathophysiology and medical treatment. Vet J. 2010; 186(1):18-24. [DOI:10.1016/j.tvjl.2010.06.011] [PMID]
- Yoshimura N, Takaoka E, Suzuki T, Kwon J. Pharmacology of the Lower Urinary Tract. In: Liao L, Madersbacher H, editors. Neurourology. Dordrecht: Springer; 2019. [DOI:10.1007/978-94-017-7509-0_8]
- Andersson KE, Pehrson R. CNS involvement in overactive bladder: Pathophysiology and opportunities for pharmacological intervention. Drugs. 2003; 63(23):2595-611. [DOI:10.2165/00003495-200363230-00003] [PMID]
- Chung AS, Cheng JN, Tse V. Psychotropic drugs and their effects on lower urinary tract function: An update. Curr Bladder Dysfunct Rep. 2016; 11:258-65. [DOI:10.1007/s11884-016-0372-5]
- Postuma RB, Gagnon JF, Tuineaig M, Bertrand JA, Latreille V, Desjardins C, et al. Antidepressants and REM sleep behavior disorder: Isolated side effect or neurodegenerative signal? Sleep. 2013; 36(11):1579-85. [DOI:10.5665/sleep.3102] [PMID]
Type of Study: case report |
Subject:
Clinical Pharmacy
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
