

Volume 11, Issue 3 (2025)
Pharm Biomed Res 2025, 11(3): 261-270 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Manasa M R, Karant C, Chandrasekhar B, K S. A Retrospective Analysis of Adverse Drug Reactions at a Tertiary Care Center–patterns, Causality, Predictability, and Preventability. Pharm Biomed Res 2025; 11 (3) :261-270
URL: http://pbr.mazums.ac.ir/article-1-688-en.html
URL: http://pbr.mazums.ac.ir/article-1-688-en.html



1- Karwar Institute of Medical Sciences
2- Department of Pharmacology, Karwar Institute of Medical Sciences, Karwar, India.
3- Department of Pharmacology, GSL Medical College and General Hospital, Rajahmundry, India.
4- Department of Pharmacology, Yadgiri Institute of Medical Sciences, Yadgiri, India.
2- Department of Pharmacology, Karwar Institute of Medical Sciences, Karwar, India.
3- Department of Pharmacology, GSL Medical College and General Hospital, Rajahmundry, India.
4- Department of Pharmacology, Yadgiri Institute of Medical Sciences, Yadgiri, India.
Full-Text [PDF 634 kb]
(414 Downloads)
| Abstract (HTML) (1198 Views)
Full-Text: (449 Views)
Introduction
All drugs inherently carry the risk of adverse reactions, and the safety concerns of drug use are highly relevant now. Adverse drug reactions (ADRs) play a significant role in the selection of drugs for the treatment of various diseases, with drugs having a better safety profile being preferred. Both healthcare professionals and the public are concerned about ADR-associated morbidity and mortality. Globally, ADRs are responsible for 0.2%-41.3% of emergency admissions, of which 28.9% are preventable [1]. The overall incidence of ADRs in India is 9.8%, while 3.4% of hospital admissions are due to ADRs and 3.7% ADRs are reported in hospitalized patients [2]. ADRs are responsible for more deaths than conditions, such as AIDS, pulmonary disease, diabetes, automobile accidents, etc [3]. Several factors related to patients, drugs, and diseases can influence the occurrence of ADRs. Age, sex, race, ethnicity, and pregnancy are examples of patient-related factors. Drug-related factors include dose, frequency, polypharmacy, while concomitant diseases are critical disease-related factors [4]. Multiple drug therapy is commonly associated with ADRs, the risk being multiplied by 1.14 with the addition of each drug [5].
ADRs can negatively impact the healthcare resources and cause economic burden to patients. ADR-associated expenses, such as hospitalization, surgery, and lost productivity, can exceed the medication expenses [6]. Thus, ADRs can impact the quality of life (QoL), result in increased physician consultations, hospitalization, and rarely death [7]. Hence, early recognition of the relationship between an ADR and a suspected drug is essential to minimize ADR-associated morbidity and mortality [8]. Good pharmacovigilance practice can minimize ADRs by early detection and effective communication, optimizing patient therapy. Evidence generated by pharmacovigilance can help regain the public trust in drugs [9]. Analysis of reported ADRs can help gather information about the ADR and patient profile, factors associated with the occurrence of ADRs, and strategies to prevent or minimize them, thus ensuring patient safety. This study aimed to assess the causality, severity, predictability, and preventability of reported ADRs using standard scales.
Materials and Methods
A retrospective observational study was conducted in Karwar Institute of Medical Sciences (KRIMS), Karwar, from April 2018 to August 2019 after obtaining Institutional ethical committee approval. All suspected ADRs reported by outpatients and inpatients of various clinical departments of KRIMS, Karwar, were collected and analyzed.
Inclusion criteria
All ADRs that were reported in out-patients and in-patients from various clinical departments of KRIMS Hospital, Karwar.
Exclusion criteria
Patients who were admitted for accidental or intentional poisoning due to drugs.
Demographic details of patients, such as age and sex, details of ADRs and the drugs/drug groups causing them, and the outcome of the ADRs were collected from suspected ADR reporting forms issued by the Indian Pharmacopoeia Commission version 1.2.
The causality of ADRs was analyzed by the World Health Organization - Uppsala monitoring Centre (WHO-UMC) scale, and ADRs were classified as certain, probable, possible, unlikely, unclassified, and unclassifiable [10]. The severity of the ADRs was assessed by the modified Hartwig and Siegel scale, which categorizes ADRs into mild, moderate, and severe [11]. The predictability of the ADRs was assessed as per Rawlins and Thompson’s classification, and ADRs were classified as type A and type B. Type A ADRs were dose dependent and predictable, whereas type B ADRs were idiosyncratic with no clear dose response relationship and hence not predictable [12]. The modified Schumock and Thornton scale was used to assess the preventability of ADRs, and the ADRs were classified as definitely preventable, probably preventable, and not preventable [13].
Statistical analysis:
Descriptive statistics were used to summarize and analyze the data, which were expressed as frequencies and percentages.
Results
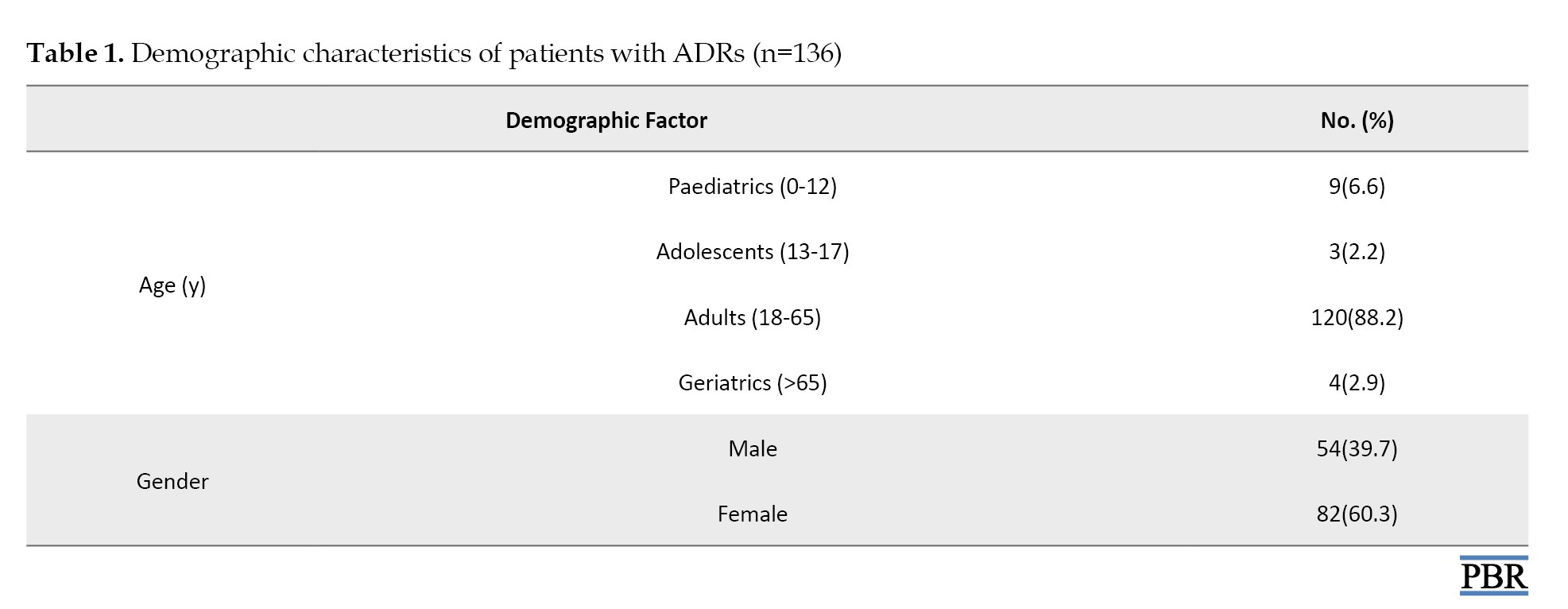
A total of 159 ADRs were reported from 136 patients from various clinical departments of KRIMS, Karwar. Most patients were adults aged between 18-65 years (88.2%). A total of 60.3% of patients were female (Table 1).
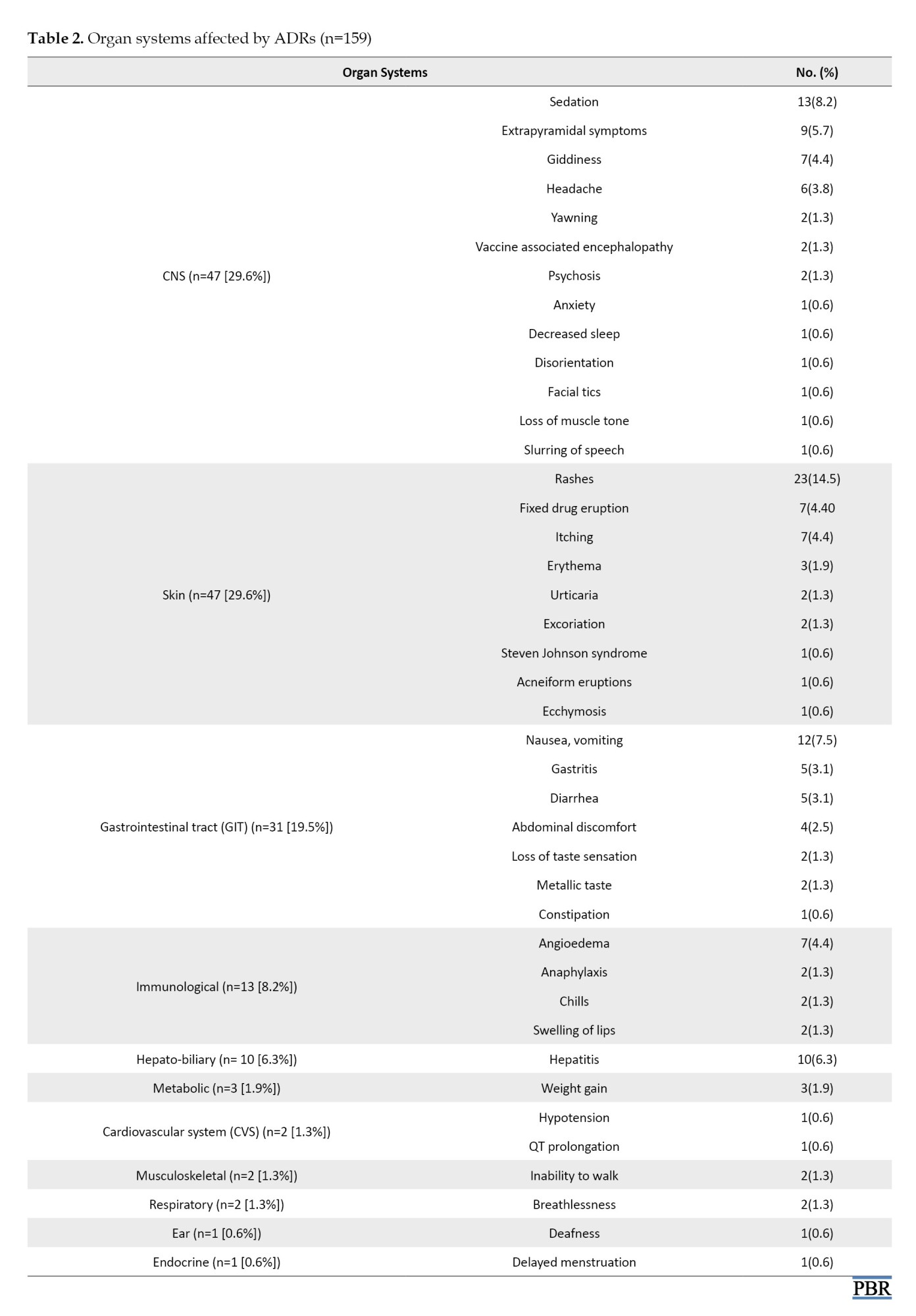
Among 159 ADRs, the skin and the central nervous system (CNS) were the predominant organ systems affected, accounting for 29.6% of ADRs each. The most common ADRs reported were rashes (14.5%) followed by sedation (8.2%), nausea, vomiting (7.5%) and hepatitis (6.3%) (Table 2).
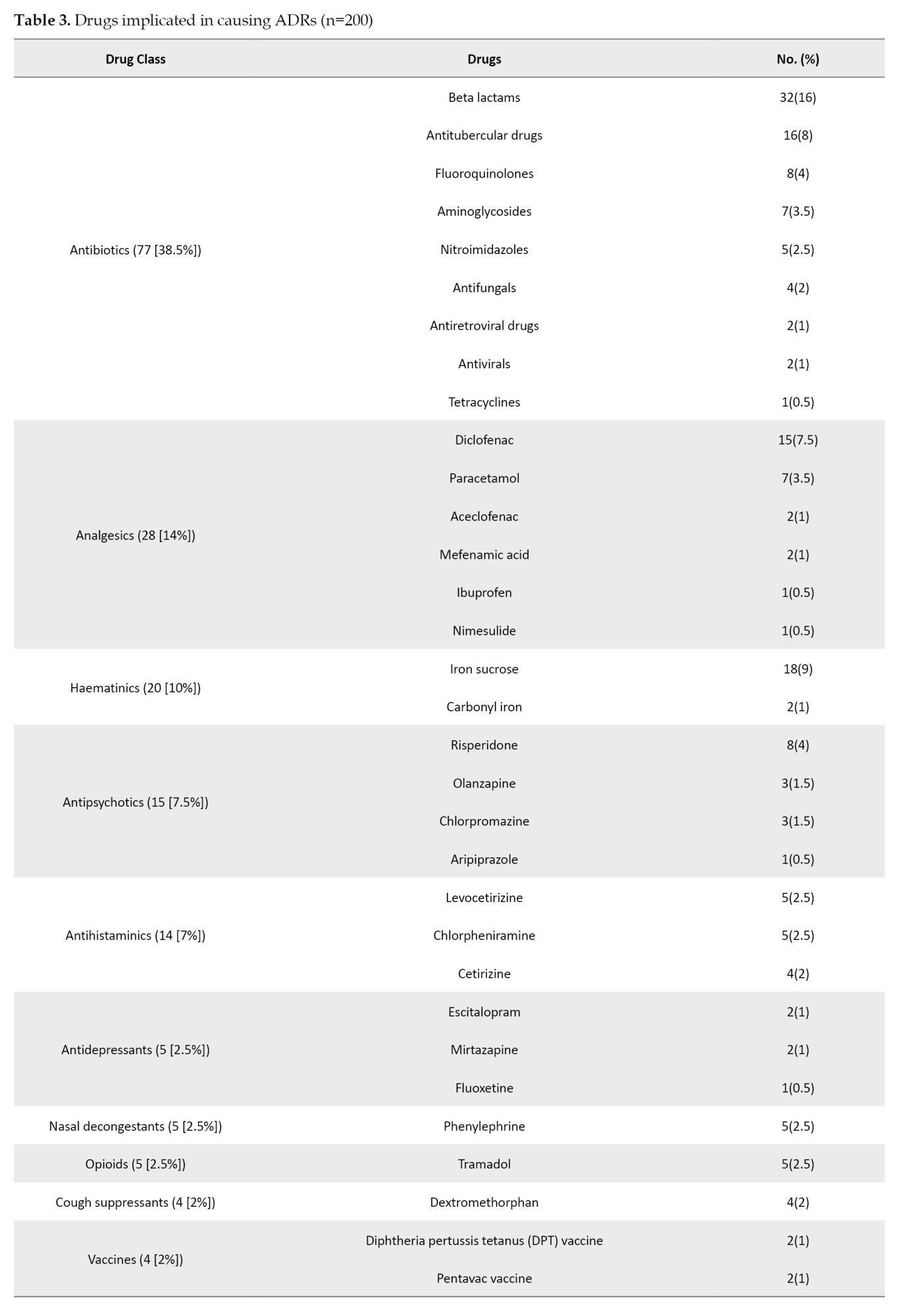
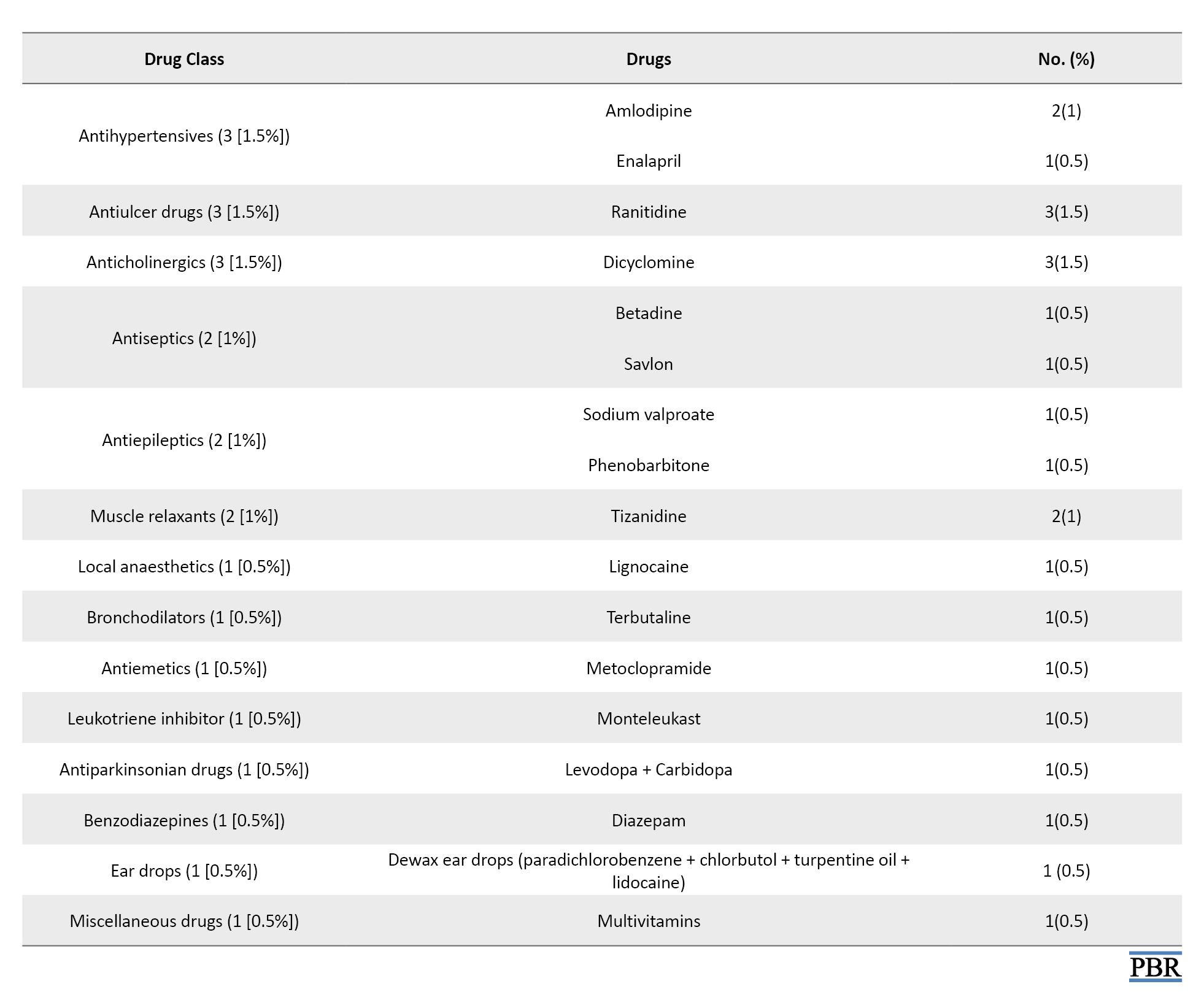
Among the 200 drugs implicated in causing the ADRs, antibiotics were most commonly involved, accounting for 38.5% of the drugs. Non-opioid analgesics were the next common class of drugs implicated (14%). Among the individual drugs, the most commonly implicated drugs were beta-lactam antibiotics (16%), followed by iron sucrose (9%) (Table 3).
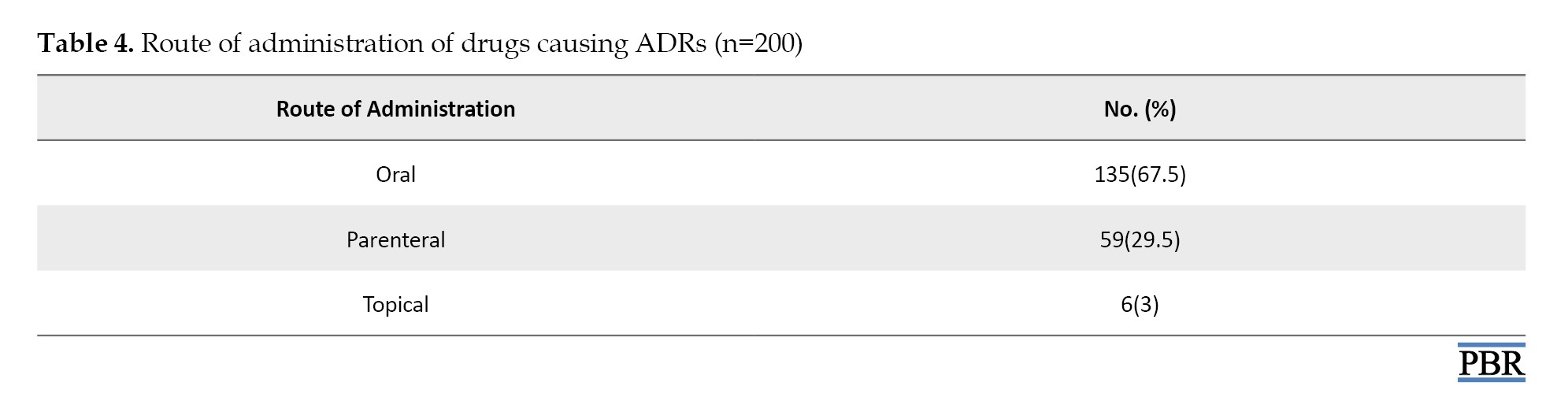
Most of the drugs causing ADRs were administered orally (67.5%), followed by parenterally (29.5%) and topically (3%) (Table 4).
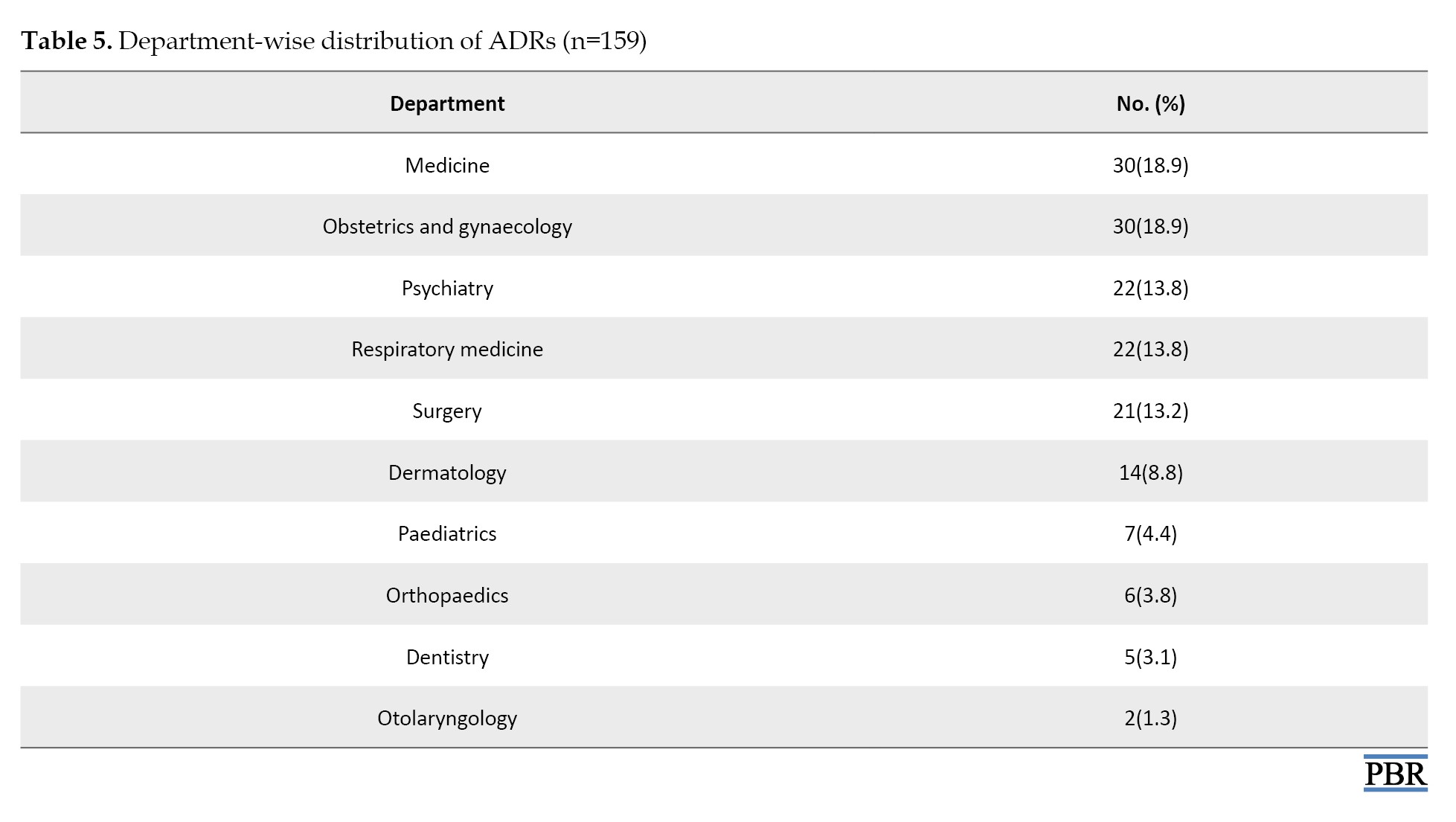
General medicine, obstetrics, and gynaecology departments reported 18.9% of ADRs (Table 5).
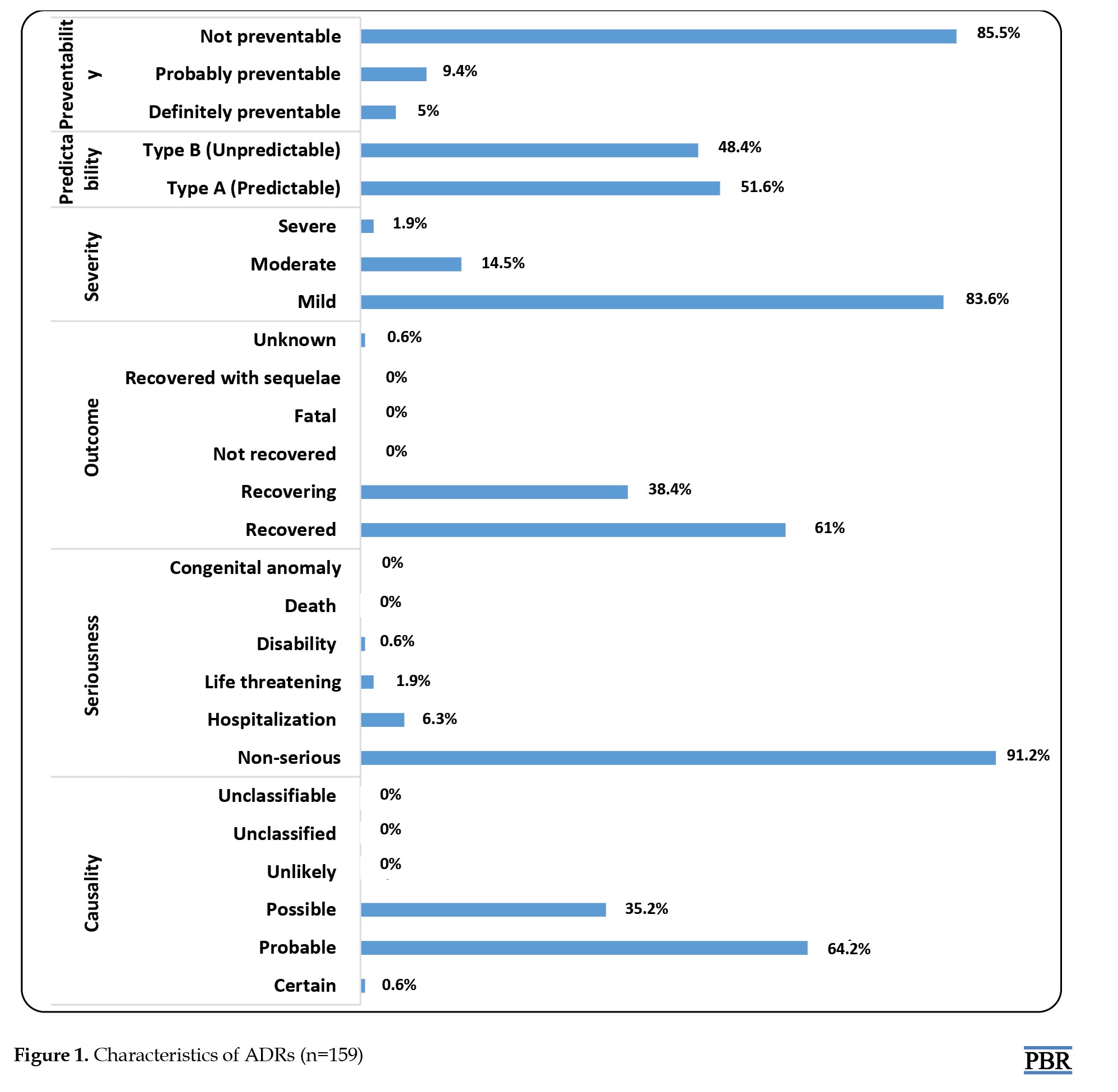
As per the WHO-UMC scale, the causality of the reported ADRs was certain at 0.6%, probably at 64.2% and possibly at 35.2% of the ADRs. Most reported ADRs were non-serious (91.2%). Among the serious ADRs, 6.3% required hospitalization, 1.9% were life-threatening, and 0.6% caused disability. A total of 61% of patients experiencing ADRs recovered, while 38.4% were recovering at the time of reporting ADRs. The outcome was unknown in 0.6% patients. According to the modified Hartwig and Siegel scale, 83.6% of ADRs were mild, 14.5% were moderate, and 1.9% were severe. As per Rawlins and Thompson’s classification, 51.6% of ADRs were predictable, and remaining (48.4%) were not predictable. According to the modified Schumock and Thornton scale, only 5% ADRs were definitely preventable, 9.4% were probably preventable, and 85.5% were not preventable (Figure 1).
All drugs inherently carry the risk of adverse reactions, and the safety concerns of drug use are highly relevant now. Adverse drug reactions (ADRs) play a significant role in the selection of drugs for the treatment of various diseases, with drugs having a better safety profile being preferred. Both healthcare professionals and the public are concerned about ADR-associated morbidity and mortality. Globally, ADRs are responsible for 0.2%-41.3% of emergency admissions, of which 28.9% are preventable [1]. The overall incidence of ADRs in India is 9.8%, while 3.4% of hospital admissions are due to ADRs and 3.7% ADRs are reported in hospitalized patients [2]. ADRs are responsible for more deaths than conditions, such as AIDS, pulmonary disease, diabetes, automobile accidents, etc [3]. Several factors related to patients, drugs, and diseases can influence the occurrence of ADRs. Age, sex, race, ethnicity, and pregnancy are examples of patient-related factors. Drug-related factors include dose, frequency, polypharmacy, while concomitant diseases are critical disease-related factors [4]. Multiple drug therapy is commonly associated with ADRs, the risk being multiplied by 1.14 with the addition of each drug [5].
ADRs can negatively impact the healthcare resources and cause economic burden to patients. ADR-associated expenses, such as hospitalization, surgery, and lost productivity, can exceed the medication expenses [6]. Thus, ADRs can impact the quality of life (QoL), result in increased physician consultations, hospitalization, and rarely death [7]. Hence, early recognition of the relationship between an ADR and a suspected drug is essential to minimize ADR-associated morbidity and mortality [8]. Good pharmacovigilance practice can minimize ADRs by early detection and effective communication, optimizing patient therapy. Evidence generated by pharmacovigilance can help regain the public trust in drugs [9]. Analysis of reported ADRs can help gather information about the ADR and patient profile, factors associated with the occurrence of ADRs, and strategies to prevent or minimize them, thus ensuring patient safety. This study aimed to assess the causality, severity, predictability, and preventability of reported ADRs using standard scales.
Materials and Methods
A retrospective observational study was conducted in Karwar Institute of Medical Sciences (KRIMS), Karwar, from April 2018 to August 2019 after obtaining Institutional ethical committee approval. All suspected ADRs reported by outpatients and inpatients of various clinical departments of KRIMS, Karwar, were collected and analyzed.
Inclusion criteria
All ADRs that were reported in out-patients and in-patients from various clinical departments of KRIMS Hospital, Karwar.
Exclusion criteria
Patients who were admitted for accidental or intentional poisoning due to drugs.
Demographic details of patients, such as age and sex, details of ADRs and the drugs/drug groups causing them, and the outcome of the ADRs were collected from suspected ADR reporting forms issued by the Indian Pharmacopoeia Commission version 1.2.
The causality of ADRs was analyzed by the World Health Organization - Uppsala monitoring Centre (WHO-UMC) scale, and ADRs were classified as certain, probable, possible, unlikely, unclassified, and unclassifiable [10]. The severity of the ADRs was assessed by the modified Hartwig and Siegel scale, which categorizes ADRs into mild, moderate, and severe [11]. The predictability of the ADRs was assessed as per Rawlins and Thompson’s classification, and ADRs were classified as type A and type B. Type A ADRs were dose dependent and predictable, whereas type B ADRs were idiosyncratic with no clear dose response relationship and hence not predictable [12]. The modified Schumock and Thornton scale was used to assess the preventability of ADRs, and the ADRs were classified as definitely preventable, probably preventable, and not preventable [13].
Statistical analysis:
Descriptive statistics were used to summarize and analyze the data, which were expressed as frequencies and percentages.
Results
A total of 159 ADRs were reported from 136 patients from various clinical departments of KRIMS, Karwar. Most patients were adults aged between 18-65 years (88.2%). A total of 60.3% of patients were female (Table 1).
Among 159 ADRs, the skin and the central nervous system (CNS) were the predominant organ systems affected, accounting for 29.6% of ADRs each. The most common ADRs reported were rashes (14.5%) followed by sedation (8.2%), nausea, vomiting (7.5%) and hepatitis (6.3%) (Table 2).
Among the 200 drugs implicated in causing the ADRs, antibiotics were most commonly involved, accounting for 38.5% of the drugs. Non-opioid analgesics were the next common class of drugs implicated (14%). Among the individual drugs, the most commonly implicated drugs were beta-lactam antibiotics (16%), followed by iron sucrose (9%) (Table 3).
Most of the drugs causing ADRs were administered orally (67.5%), followed by parenterally (29.5%) and topically (3%) (Table 4).
General medicine, obstetrics, and gynaecology departments reported 18.9% of ADRs (Table 5).
As per the WHO-UMC scale, the causality of the reported ADRs was certain at 0.6%, probably at 64.2% and possibly at 35.2% of the ADRs. Most reported ADRs were non-serious (91.2%). Among the serious ADRs, 6.3% required hospitalization, 1.9% were life-threatening, and 0.6% caused disability. A total of 61% of patients experiencing ADRs recovered, while 38.4% were recovering at the time of reporting ADRs. The outcome was unknown in 0.6% patients. According to the modified Hartwig and Siegel scale, 83.6% of ADRs were mild, 14.5% were moderate, and 1.9% were severe. As per Rawlins and Thompson’s classification, 51.6% of ADRs were predictable, and remaining (48.4%) were not predictable. According to the modified Schumock and Thornton scale, only 5% ADRs were definitely preventable, 9.4% were probably preventable, and 85.5% were not preventable (Figure 1).
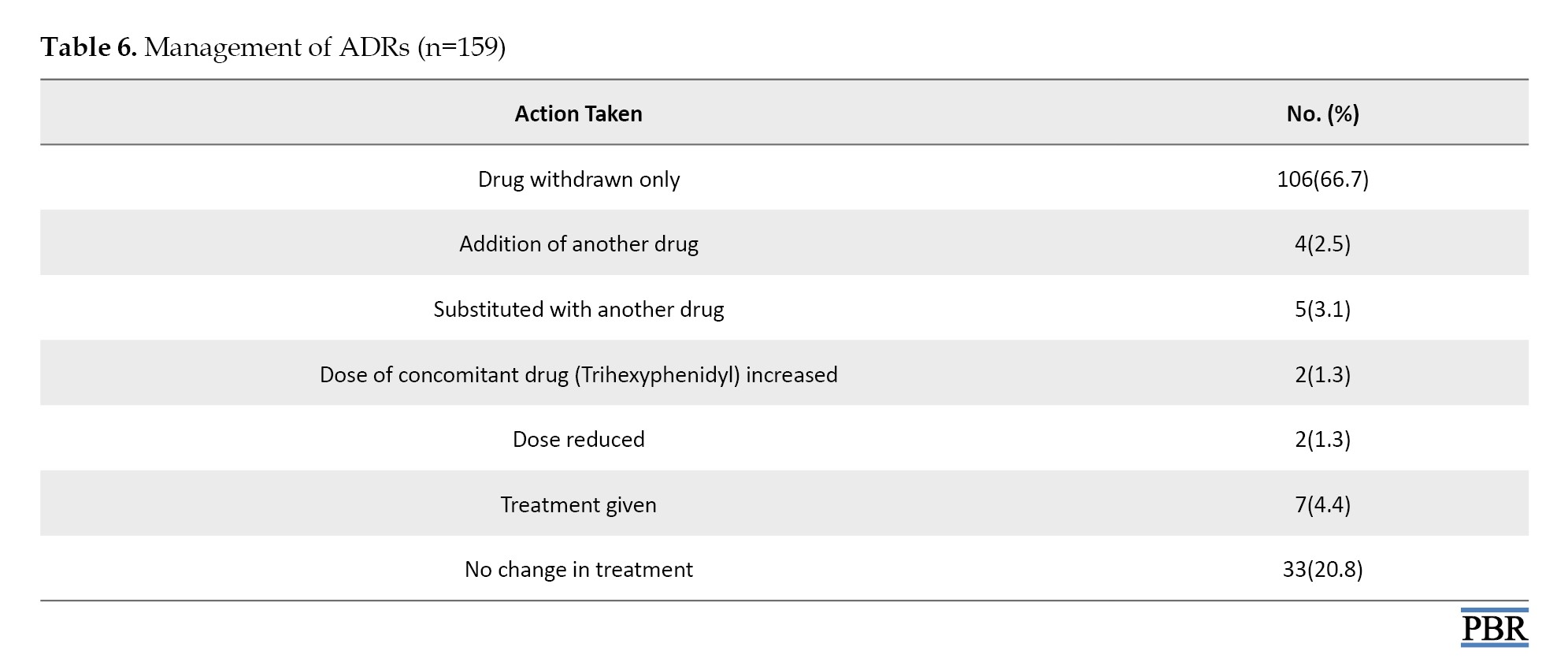
The majority of ADRs subsided after withdrawing the offending drug (66.7%). Treatment was required for only 4.4% of the ADRs. Treatment was not changed in 20.8% (Table 6).
Discussion
ADRs are associated with significant morbidity and mortality. Early recognition of ADRs plays a key role in their effective management. Analysis of reported ADRs helps identify various drug, disease, and patient-related risk factors, thereby helping in the prevention of future ADRs. Hence, we conducted this retrospective observational study to analyze the causality, severity, seriousness, predictability and preventability of reported ADRs.
In our study, 159 ADRs were reported from 136 patients. Our study showed a female preponderance. This is consistent with the findings of Prajapati et al [14], but contrasting findings were reported by Gupta et al [15] and Bhattacharjee et al. [16]. However, Singh et al. reported equal occurrence of ADRs in males and females [17]. Thus, it can be concluded that gender does not play a role in the occurrence of ADRs. Most of our study population were adults aged 18-65 (88.2%). Similar observations were reported by Behera et al. [18] and Bhandare et al. [19].
In our study, the skin and the central nervous system (CNS) were the predominant organ systems affected, accounting for 29.6% of ADRs each. Patidar et al. [20] and Agrawal et al. [21] also reported that skin was the most commonly affected by ADRs. The most common ADRs reported in our study were rashes (14.5%), followed by sedation (8.2%), nausea, vomiting (7.5%), and hepatitis (6.3%). Many studies have reported that rash was the commonest ADR manifestation [22, 23]. This could be because skin is the largest organ system, and skin lesions can be easily identified.
In the current study, antibiotics were the most commonly involved drug class (38.5%), followed by non-opioid analgesics (14%). Among the individual drugs, beta-lactam antibiotics were most commonly implicated (16%). Kaur et al. [24] and Keche et al. [25] also reported similar findings.
In our study, most of the drugs causing ADRs were administered orally (67.5%). This is consistent with the study by Shamna et al. [26]. However, Pathak et al. reported that the majority of drugs causing ADRs were administered by the intravenous route [27] and Lihite et al. reported that drugs applied topically were commonly responsible [28]. The departments that reported the majority of ADRs were General Medicine and Obstetrics and Gynaecology (18.9% each). Venkatasubbaiah et al. also reported that the General Medicine Department contributed the majority of the ADRs [29] However, many studies have reported that the dermatology department reported most of the ADRs [24, 28]. All the ADRs in our study were reported by doctors. Badyal et al. also reported similar findings [30]. However, Singh et al. reported that doctors contributed most of the ADRs, followed by nursing staff and patients [31]. It is the professional obligation of all healthcare professionals – doctors, nurses, dentists, and pharmacists- to report ADRs. However, underreporting is common.
As per the WHO-UMC scale, the causality of the majority of reported ADRs was probable. This is consistent with Ramnath et al [32] The reason for this trend may be polypharmacy. Most of the reported ADRs were non-serious (91.2%), which is consistent with a study by Sen et al. [33]. According to the modified Hartwig and Siegel scale, severity of majority of ADRs was mild (83.6%). Similar findings were reported by James et al. [34] But Sudha et al. reported moderate severity of majority of ADRs [35].
As per the Rawlins and Thompson’s classification, most ADRs were predictable (51.6%). Singh et al. also reported similar findings [17]. According to the modified Schumock and Thornton scale, 85.5% of reported ADRs were not preventable. This is consistent with the study by Vemuri et al. [36] This may be because majority of the patients did not have a history of allergy and most of the drugs causing ADRs did not require monitoring.
At the time of reporting of ADRs, most patients experiencing ADRs had recovered. Most ADRs subsided after withdrawing the offending drug (66.7%). Treatment was required for only 4.4% of the ADRs. This is consistent with the study by Tongaonkar et al. [37].
Conclusion
ADRs are a common cause of morbidity and mortality. However, underreporting is rampant. Early detection of the causal relationship between drugs and adverse reactions is crucial for effective management, as most ADRs subside after withdrawal of the offending drug. Prompt detection of ADRs can decrease the patient morbidity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Ethics Committee of Karwar Institute of Medical Sciences, Karwar, India (Code: IEC/KRIMS/O/48/2019-20).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed significantly to the work’s conception, design, data acquisition, analysis, or interpretation, drafting or critically revising for intellectual content, final approval of the version to be published, accountability for all work aspects, ensuring integrity, and resolving questions.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the Clinical Faculty of Karwar Institute of Medical Sciences, Karwar, India, for their help and support in conducting this study.
References
Discussion
ADRs are associated with significant morbidity and mortality. Early recognition of ADRs plays a key role in their effective management. Analysis of reported ADRs helps identify various drug, disease, and patient-related risk factors, thereby helping in the prevention of future ADRs. Hence, we conducted this retrospective observational study to analyze the causality, severity, seriousness, predictability and preventability of reported ADRs.
In our study, 159 ADRs were reported from 136 patients. Our study showed a female preponderance. This is consistent with the findings of Prajapati et al [14], but contrasting findings were reported by Gupta et al [15] and Bhattacharjee et al. [16]. However, Singh et al. reported equal occurrence of ADRs in males and females [17]. Thus, it can be concluded that gender does not play a role in the occurrence of ADRs. Most of our study population were adults aged 18-65 (88.2%). Similar observations were reported by Behera et al. [18] and Bhandare et al. [19].
In our study, the skin and the central nervous system (CNS) were the predominant organ systems affected, accounting for 29.6% of ADRs each. Patidar et al. [20] and Agrawal et al. [21] also reported that skin was the most commonly affected by ADRs. The most common ADRs reported in our study were rashes (14.5%), followed by sedation (8.2%), nausea, vomiting (7.5%), and hepatitis (6.3%). Many studies have reported that rash was the commonest ADR manifestation [22, 23]. This could be because skin is the largest organ system, and skin lesions can be easily identified.
In the current study, antibiotics were the most commonly involved drug class (38.5%), followed by non-opioid analgesics (14%). Among the individual drugs, beta-lactam antibiotics were most commonly implicated (16%). Kaur et al. [24] and Keche et al. [25] also reported similar findings.
In our study, most of the drugs causing ADRs were administered orally (67.5%). This is consistent with the study by Shamna et al. [26]. However, Pathak et al. reported that the majority of drugs causing ADRs were administered by the intravenous route [27] and Lihite et al. reported that drugs applied topically were commonly responsible [28]. The departments that reported the majority of ADRs were General Medicine and Obstetrics and Gynaecology (18.9% each). Venkatasubbaiah et al. also reported that the General Medicine Department contributed the majority of the ADRs [29] However, many studies have reported that the dermatology department reported most of the ADRs [24, 28]. All the ADRs in our study were reported by doctors. Badyal et al. also reported similar findings [30]. However, Singh et al. reported that doctors contributed most of the ADRs, followed by nursing staff and patients [31]. It is the professional obligation of all healthcare professionals – doctors, nurses, dentists, and pharmacists- to report ADRs. However, underreporting is common.
As per the WHO-UMC scale, the causality of the majority of reported ADRs was probable. This is consistent with Ramnath et al [32] The reason for this trend may be polypharmacy. Most of the reported ADRs were non-serious (91.2%), which is consistent with a study by Sen et al. [33]. According to the modified Hartwig and Siegel scale, severity of majority of ADRs was mild (83.6%). Similar findings were reported by James et al. [34] But Sudha et al. reported moderate severity of majority of ADRs [35].
As per the Rawlins and Thompson’s classification, most ADRs were predictable (51.6%). Singh et al. also reported similar findings [17]. According to the modified Schumock and Thornton scale, 85.5% of reported ADRs were not preventable. This is consistent with the study by Vemuri et al. [36] This may be because majority of the patients did not have a history of allergy and most of the drugs causing ADRs did not require monitoring.
At the time of reporting of ADRs, most patients experiencing ADRs had recovered. Most ADRs subsided after withdrawing the offending drug (66.7%). Treatment was required for only 4.4% of the ADRs. This is consistent with the study by Tongaonkar et al. [37].
Conclusion
ADRs are a common cause of morbidity and mortality. However, underreporting is rampant. Early detection of the causal relationship between drugs and adverse reactions is crucial for effective management, as most ADRs subside after withdrawal of the offending drug. Prompt detection of ADRs can decrease the patient morbidity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Institutional Ethics Committee of Karwar Institute of Medical Sciences, Karwar, India (Code: IEC/KRIMS/O/48/2019-20).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed significantly to the work’s conception, design, data acquisition, analysis, or interpretation, drafting or critically revising for intellectual content, final approval of the version to be published, accountability for all work aspects, ensuring integrity, and resolving questions.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the Clinical Faculty of Karwar Institute of Medical Sciences, Karwar, India, for their help and support in conducting this study.
References
- World Health Organization. Safety of medicines: A guide to detecting and reporting adverse drug reactions why health professionals need to take action. Geneva: World Health Organization; 2002. [Link]
- Arulmani R, Rajendran SD, Suresh B. Adverse drug reaction monitoring in a secondary care hospital in South India. Br J Clin Pharmacol. 2008; 65(2):210-6. [DOI:10.1111/j.1365-2125.2007.02993.x] [PMID]
- Mangla R, Verma S, Gupta MC, Singhal S. Adverse drug reaction monitoring of commonly prescribed medicines in gynaecology patients in a tertiary care hospital in North India. Int J Health Sci Res. 2017; 7(11):111-7. [Link]
- Patiyal N, Gautam A, Kansal D, Sood A, Chauhan A, Bodh S. Pattern of adverse drug effects reported by patients being treated in a tertiary healthcare institution in North India: A retrospective observational study. IP Int J Comprehensive Adv Pharmacol. 2022; 7(2):87-90. [DOI:10.18231/j.ijcaap.2022.016]
- Singh H, Dulhani N, Kumar BN, Singh P, Tewari P, Nayak K. A Pharmacovigilance study in medicine department of tertiary care hospital in Chhattisgarh (Jagdalpur), India. J Young Pharm. 2010; 2(1):95-100. [DOI:10.4103/0975-1483.62222] [PMID]
- World Health Organization. Medicines: Safety of medicines - adverse drug reactions. Geneva: WHO; 2008. [Link]
- Agada PO, Eyong AK, Asukwo EO, Irene C. Incidence of adverse drug reactions in patients on antiretroviral therapy: a study of pharmaceutical care in HIV interventions in a tertiary health facility in southern Nigeria. Res Human Soc Sci. 2016; 6(14):103-7. [Link]
- Joseph SG, Badyal DK. Spontaneous adverse drug reaction monitoring in a tertiary care hospital in Northern India. JK Sci. 2016; 18(2):103-6. [Link]
- World Health Organization. The safety of medicines in public health programmes: Pharmacovigilance an essential tool. Geneva: World Health Organization; 2006. [Link]
- World Health Organization. The Use of the WHO-UMC System for Standardised Case Causality Assessment. Geneva: World Health Organization; 2013. [Link]
- Hartwig SC, Siegel J, Schneider PJ. Preventability and severity assessment in reporting adverse drug reactions. Am J Hosp Pharm. 1992; 49:2229-32. [DOI:10.1093/ajhp/49.9.2229] [PMID]
- Raut AL, Patel P, Patel C, Pawar A. Preventability, predictability and seriousness of adverse drug reactions amongst medicine inpatients in a teaching hospital: A prospective observational study. Int J Pharm Chem Sci. 2012; 1(3):1293-9.[Link]
- Schumock GT, Thornton JP. Focusing on the preventability of adverse drug reactions. Hosp Pharm. 1992; 27(6):538. [PMID]
- Prajapati H, Kansal D, Chaudhary UK. Pattern of adverse drug reactions in rural tertiary care medical college and hospital of Himachal Pradesh: A retrospective observational study. Indian J Pharm Pharmacol. 2018; 5(1):4-6. [DOI:10.18231/2393-9087.2018.0002]
- Gupta A, Kaur A, Shukla P, Chhabra H. Adverse Drug Reactions pattern in a tertiary level teaching hospital: A Retrospective Study. Indian J Pharm Pract. 2017; 10(1):27-31. [Link]
- Bhattacharjee P, Das L, Ghosh R, Lalromawii, Das UK. Pattern of adverse drug reactions reported at a tertiary health care teaching hospital of Tripura: A retrospective study. Int J Basic Clin Pharmacol. 2016; 5(4):1293-99. [DOI:10.18203/2319-2003.ijbcp20162177]
- Singh A, Jain A, Soni M, Shukla P, Lahon J, Verma AK. Pattern of adverse drug reactions reported at a tertiary care teaching hospital in northern India. Int J Basic Clin Pharmacol. 2020; 9(4)625-32. [DOI:10.18203/2319-2003.ijbcp20201189]
- Behera SK, Rath B, Biswal SB, Mohapatra S. Pattern of adverse drug reactions in a tertiary care hospital in Western Odisha. Int J Pharm Sci Res. 2018; 9(6):2471-7. [Link]
- Bhandare B, Shabeer D, Satyanarayana V. A study on adverse drug reactions in a tertiary care hospital in Bangalore. Indian J Pharm Pharmacol. 2017; 4(1):49-54. [Link]
- Patidar D, Rajput MS, Nirmal NP, Savitri W. Implementation and evaluation of adverse drug reaction monitoring system in a tertiary care teaching hospital in Mumbai, India. Interdiscip Toxicol. 2013; 6(1):41-6. [DOI:10.2478/intox-2013-0008] [PMID]
- Agrawal M, Hishikar R, Joshi U, Halwai A, Toddar TL, Khubchandani V. Adverse drug reaction scenario at ADR Monitoring Centre of Tertiary Teaching Hospital at Raipur. Indian J Pharm Pharmacol. 2015; 2(3):169-75. [Link]
- Khan LM, Al-Harthi SE, Saadah OI. Adverse drug reactions in hospitalized pediatric patients of Saudi Arabian University Hospital and impact of pharmacovigilance in reporting ADR. Saudi Pharm J. 2013; 21(3):261-6. [DOI:10.1016/j.jsps.2012.09.004] [PMID]
- Bhabhor PH, Patel TK, Vahora R, Patel PB, Desai N. Adverse drug reactions in a tertiary care teaching hospital in India: Analysis of spontaneously reported cases. Int J Basic Clin Pharmacol. 2017; 3(6):1078-85. [DOI:10.5455/2319-2003.ijbcp20141228]
- Kaur M, Deb T, Kairi J, Arora A. A pharmacovigilance study of adverse drug reactions in a tertiary care hospital in Haryana. Int J Basic Clin Pharmacol. 2019; 8(10):2184–90.[DOI:10.18203/2319-2003.ijbcp20194149]
- Keche Y, Gaikwad N, Dhaneria S. Preventability, predictability, severity and causality assessment of adverse drug reactions reported from a teaching hospital in chhattisgarh: A retrospective analysis. J Family Med Prim Care. 2021; 10(7):2541-5. [DOI:10.4103/jfmpc.jfmpc_2374_20] [PMID]
- Shamna M, Dilip C, Ajmal M, Linu PM, Shinu C, Jafer CP, et al. A prospective study on Adverse Drug Reactions of antibiotics in a tertiary care hospital. Saudi Pharm J. 2014; 22(4):303-8. [PMID]
- Pathak AK, Kumar M, Dokania S, Mohan L, Dikshit H. A retrospective analysis of reporting of adverse drug reactions in a Tertiary Care Teaching Hospital: One Year Survey. J Clin Diagn Res. 2016; 10(8):FC01-4. [DOI:10.7860/JCDR/2016/18826.8284] [PMID]
- Lihite RJ, Lahkar M, Das S, Hazarika D, Kotni M, Maqbool M, et al. A study on adverse drug reactions in a tertiary care hospital of Northeast India. Alexandria J Med. 2017; 53(2):151-6. [DOI:10.1016/j.ajme.2016.05.007]
- Venkatasubbaiah M, Reddy PD, Satyanarayana SV. Analysis and reporting of adverse drug reactions at a tertiary care teaching hospital Alexandria J Med. 2018; 54(4):597-603. [DOI:10.1016/j.ajme.2018.10.005]
- Badyal DK, Kanish B, Gulrez G. Causality assessment and pattern of adverse drug reactions in a tertiary care hospital. Int J Basic Clin Pharmacol. 2018; 7(2):210-4. [DOI:10.18203/2319-2003.ijbcp20180089]
- Singh P, Agrawal M, Hishikar R, Joshi U, Maheshwari B, Halwai A. Adverse drug reactions at adverse drug reaction monitoring center in Raipur: Analysis of spontaneous reports during 1 year. Indian J Pharmacol. 2017; 49(6):432-7. [DOI:10.4103/ijp.IJP_781_16] [PMID]
- Ramnath SN, Nair PV, Philip MM, Palappallil DS. Adverse drug reactions reported to an ADR monitoring centre as a part of the Pharmacovigilance Programme of India: A retrospective analysis of 3-year data. Natl J Physiol Pharm Pharmacol. 2023; 13(09):1893-7. [DOI:10.5455/njppp.2023.13.07344202323072023]
- Sen M, Singh A, Misra M. Retrospective analysis of adverse drug reactions reported at ADR monitoring centre under PvPI in a tertiary care hospital. Int J Basic Clin Pharmacol. 2018; 7(2):303–8. [DOI:10.18203/2319-2003.ijbcp20180103]
- James J, Rani J. A prospective study of adverse drug reactions in a tertiary care hospital in South India. Asian J Pharm Clin Res. 2020; 13(1):89-92. [DOI:10.22159/ajpcr.2020.v13i1.36028]
- Sudha TYS, Vangoori Y, Varghese AV. A profile of adverse drug reactions in a tertiary care teaching hospital and associated factors. Biomed Pharmacol J. 2021; 14(1):367-71. [DOI:10.13005/bpj/2135]
- Vemuri VR. A retrospective and observational study of the adverse drug reactions reported in a tertiary care hospital. Int J Basic Clin Pharmacol. 2024; 13(2):213-8. [DOI:10.18203/2319-2003.ijbcp20240033]
- Tongaonkar A, Joshi K, Mulkalwar A, Dagli S. Clinical profile of adverse drug reactions in patients admitted to internal medicine wards of a tertiary care hospital. Int J Acad Med. 2023; 9(4):185-91. [DOI:10.4103/ijam.ijam_18_23]
Type of Study: Original Research |
Subject:
Pharmacology
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
