

Volume 9, Issue 3 (2023)
Pharm Biomed Res 2023, 9(3): 231-242 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hatem G, Awarkeh A, Jaffal L H, Khachman D, Al-Hajje A, Zein S. Drug-related Problems Among Type 2 Diabetic Patients With Hypertension in a Tertiary Care Hospital in Lebanon: A Cross-sectional Study. Pharm Biomed Res 2023; 9 (3) :231-242
URL: http://pbr.mazums.ac.ir/article-1-524-en.html
URL: http://pbr.mazums.ac.ir/article-1-524-en.html



1- Clinical and Epidemiological Research Laboratory, Faculty of Pharmacy, Lebanese University, Hadat, Lebanon.
Full-Text [PDF 783 kb]
(1036 Downloads)
| Abstract (HTML) (2220 Views)
Full-Text: (1429 Views)
Introduction
The prevalence of type 2 diabetes (T2D) have significantly increased, having upward trend [1] and high clinical and public health burden [2]. There are several modifiable risk factors for T2D. Adequate management of these risk factors can reduce mortality and the occurrence of comorbidities [3]. T2D is associated with an increased risk of cardiovascular diseases (CVD) such as myocardial infarction, ischemic stroke, heart failure, and aortic valve stenosis [4]. Drug-related problems are common among T2D patients and can negatively affect their quality of life [5]. The T2D patients with hypertension are at a higher risk of drug-related problems (DRPs), considering the number of medications used for their treatment [6]. These problems can induce mortality and morbidity among patients and extend their hospitalization due to the challenges in controlling their blood pressure and the diabetes-related complications [7].
The DRPs can be prevented [8] and lead to significantly lower health expenditures [9]. Several factors can increase the risk of DRPs in T2D patients with hypertension. The main reported factors are polypharmacy, older age, and underlying diseases [10]. A recent cross-sectional study found that, for every one unit increase in the number of medications, the odds of DRPs increased by 10% [11]. Inappropriate prescribing, over-the-counter drug use, and low adherence to treatment can also increase the risk of DRPs [12]. Older patients are more prone to DRPs and require interventions to manage some problems, such as the use of expired medications and drug storage issues [13]. Inpatients and those with many chronic conditions are also at a higher risk of developing DRPs [14].
A recent study investigated DRPs among T2D patients in Lebanon [15]. However, no study was found on hospitalized T2D patients with hypertension in Lebanon. There are few studies investigated them in other countries. Understanding DRPs can help make informed health decisions and effectively manage these patients. Therefore, this study aims to investigate DRPs and their causes among T2D patients with hypertension and to find the predictors of these problems.
Materials and Methods
Study design and samples
This is an observational cross-sectional study that was conducted for six months (March-September 2021) on patients diagnosed with T2D and hypertension admitted to the internal medicine department of a tertiary care hospital in Lebanon. Adult patients receiving one or more anti-diabetes drugs and at least one medication for CVD or hypertension were included. The criteria based on sex, age, and ethnicity were not used. The sample size was determined using the Epi Info software, version 7. Based on findings from a previous study [16], 90.5% of T2D patients had at least one DRP. Considering a 95% confidence interval and a 5% margin of error, the minimum sample size was 133.
Data collection
After explaining the study objectives orally to the patients for 15 minutes and inviting them to participate in the study, their written informed consent was obtained. For surveying their characteristics, a questionnaire was developed in English based on the literature review [14, 17]. It was tested in a pilot study on 10 patients, and the items that needed more clarity were either modified or deleted. The adequacy of the instrument was examined based on a technique recommended in a previous study [18]. Positive inter-item correlations [ranging 0.25-0.35), test re-test reliability of 0.807, and a Cronbach α of 0.737 were obtained, indicating the adequacy of the designed questionnaire. The first part surveys the general characteristics of participants such as sex, age (<65 or ≥65), height, weight, educational level (illiterate, primary school, secondary school, academic), employment status, marital status, medical insurance coherence, and lifestyle habits such as smoking, alcohol and coffee consumption, physical activity and its frequency, and the recommended type of diet (low-carbohydrates, low-salt, or low-fat). The second part surveys the medical and medication history: Duration of diabetes and CVD, glycosylated hemoglobin A1C (HbA1C) level (target level <7%) [19], other associated diseases, name, dosage, and administration of used medications, and the reason for hospitalization.
Based on the information obtained by the instruments as well as those extracted from the patients’ medical records, effectiveness of diabetes and CVD treatment, drug indication, drug contraindication, drug dosage, drug combinations, and adverse drug reactions (ADR) were evaluated [20-22]. The Pharmaceutical Care Network Europe (PCNE) classification system, version 7 was used to categorize the DRPs [23]. Three domains of problems (treatment effectiveness, adverse safety, and other) and three domains of causes (drug selection, dose selection, and other) based on the PCNE classification were assessed.
Statistical analysis
Statistical analyses were performed in SPSS software, version 27 (SPSS Inc, Chicago, Illinois). Based on the values of the skewness (0.027) and kurtosis (0.470), the data were found to have normal distribution and met the expected values [24]. The body mass index (BMI) of patients was calculated by dividing the weight (in kilograms) by the height (in meters squared). Then, the patients were categorized based on BMI according to the recommended criteria [25]. Categorical variables were presented by frequency and percentage. The data related to age, duration of diabetes and other comorbidities, and number of drugs per patient were described by Mean±SD. Bivariate analysis was conducted on the dichotomous dependent variable (DRPs). Independent-sample t-test was performed over continuous independent variables, and chi-square/Fisher’s exact test were used for categorical variables. Binary logistic regression was done on the two most frequent DRPs producing odd ratios (ORs) at a 95% confidence interval (CI). The Risk factors with P<0.20 were in bivariate analyses. A P<0.05 was considered statistically significant. The statistical model for finding the predictors of non-optimal treatment effect had a P<0.001 in Omnibus test, (Nagelkerke R square=0.411). The model for finding the predictors of an untreated indication also had a P<0.001 in Omnibus test (Nagelkerke R square=0.919).
Results
General characteristics of the patients
Overall, 146 eligible patients participated, out of whom 135(92.5%) completed the survey. Table 1 represents their general characteristics and lifestyle. Most of them were female (57% vs. 43% male). Their mean age was 70.2±11.1 years; 100(74.1%) <65 years, and 35 (25.9%) ≥65 years. About 25% of patients had a normal BMI; most of them were overweight (31.9%) or obese (40%). Most patients were married (60.7%) and illiterate (47.4%) or with a primary school education (35.6%). Almost 80% were unemployed, and 92.6% had a family caregiver. Regards lifestyle factors, only 23.7% were smokers; 20.7% had physical activity for less than 150 minutes per week, and 67.4% were coffee consumers. Low-carbohydrate, low-salt, or low-fat diets were adopted by about one-third of patients
Medical and medication history

Table 2 shows the statistics for medical and medication history of the patients. Most of patients (64.4%) had been hospitalized for seven days or less. Hospitalization rate related to diabetes and CVD was 17.0% and 26.7%, respectively. The mean duration of diabetes was 12.5±7.8 years, and only 38.6% achieved the target level of HbA1C. Retinopathy was the most common associated complication (57.0%), followed by diabetic foot (17.0%). The mean duration of hypertension was 10.0±7.0 years. The CVDs were coronary artery disease (62.2%), heart failure (13.3%), and stroke (11.9%). Other comorbidities were renal insufficiency (77.0%) and dyslipidemia (20.0%). Sixty percentage of patients were treated by insulin alone in the hospital, and the rest (40%) by combination of insulin and oral antidiabetics including dipeptidyl peptidase-4 (DPP4) inhibitors (24.4%) and metformin (23.7%). The most common antihypertensive and CVD drugs were beta blockers (69.6%), antiplatelet agents (63.7%), lipid-lowering drugs (57.8%), and diuretics (49.6%).


Drug-related problems and causes
The identified DRPs and their causes are presented in Table 3. The most reported problems were related to treatment effectiveness (88.1%). Most of these problems were related to the non-optimal effect of drug treatment (48.2%), and untreated indication (38.3%). The causes of these problems were primarily related to drug selection or dose selection (72.0% and 21.8%, respectively). One of the reported causes was the lack of receiving a synergistic medication (46.0%). In this study, 31 patients did not receive angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB), despite having a history of atherosclerotic CVD or microalbuminuria. The absence of primary or secondary prevention of CVD without contraindication was also reported in patients with lower limb edema. Moreover, 12 patients received moderate-intensity statin instead of high-intensity statin. Other patients received inadequate medications (enoxaparin, saxagliptin, trandolapril, and moxonidine). The most prescribed drugs in the presence of contraindication were six moxonidine cases with a creatinine clearance (ClCr) <30 mL/min, two metformin cases (ClCr <30 mL/min), and three trimetazidine cases (ClCr <30 mL/min, Parkinson disease). Other problems were also reported such as hypotension (due to the combination of several antihypertensive drugs), hyperkalemia, hyponatremia (due to the combination of diuretics), and hypoglycemia (due to insulin). Serum creatinine level was significantly higher in patients who had DRPs (1.35 vs. 0.94 mg/dL; P=0.004) and those with the problem “non-optimal effect of drug treatment” (1.44 vs. 1.07 mg/dL; P=0.006).

Predictors of DRPs
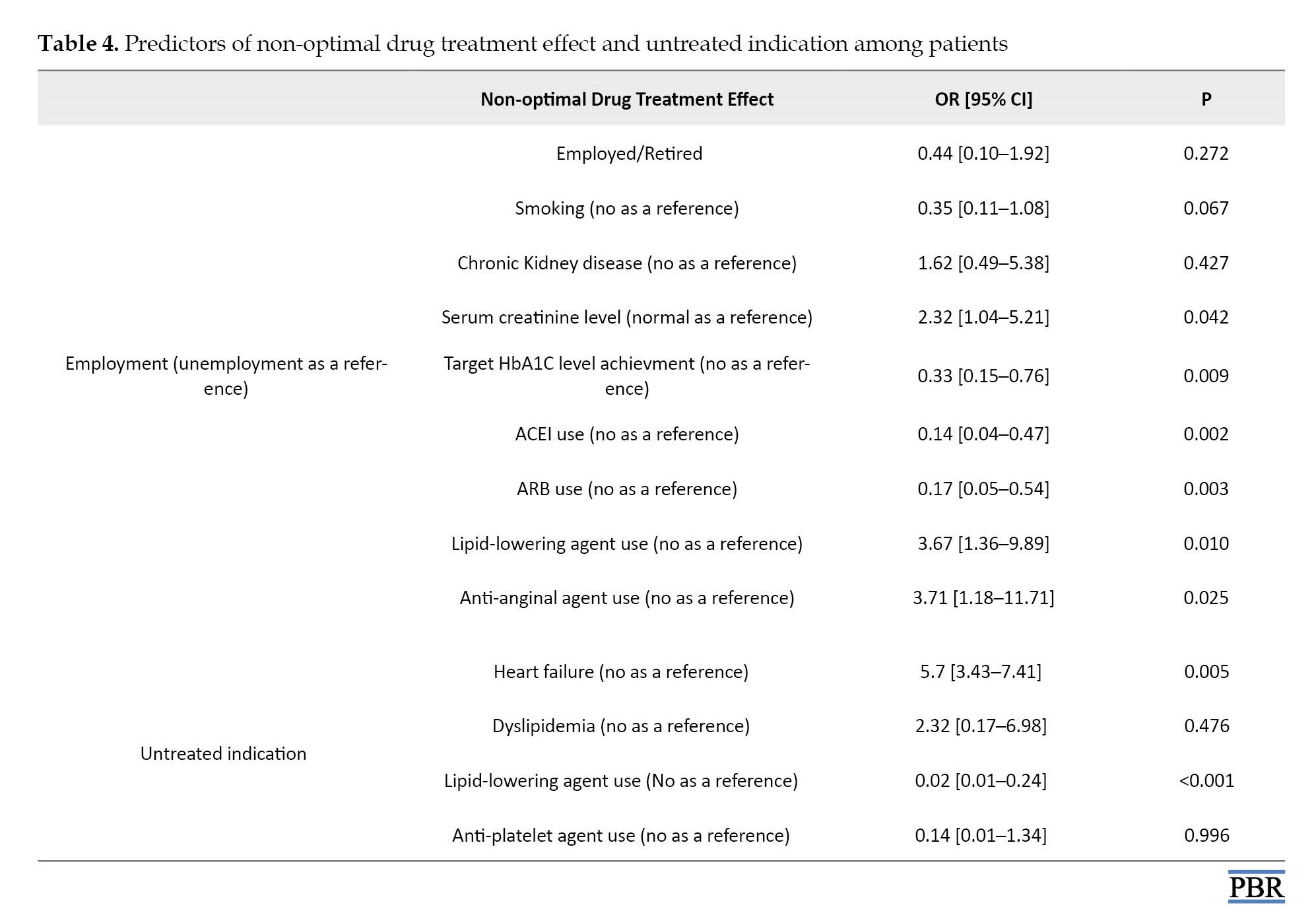
Table 4 presents the predictors of non-optimal treatment effect and the existence of an untreated indication. After adjusting the effect of covariates, the odds of non-optimal drug treatment effect were 2.32 times higher for patients with elevated serum creatinine level compared to those with normal values (OR=2.32; 95% CI, 1.04%-5.21%; P=0.042). These odds were also higher if patients used lipid-lowering agents (OR=3.67; 95% CI, 1.36%-9.89%; P=0.010) or anti-anginal agents (OR=3.71; 95% CI, 1.18%-11.71%; P=0.025), compared to non-users. Moreover, the odds of non-optimal treatment effect were 67% lower among patients with an achieved HbA1C target level compared to those with abnormal levels (OR=0.33; 95% CI, 0.15%-0.76%; P=0.009). They were also lower among patients using ACEIs (OR=0.14; 95% CI: 0.04-0.47; P=0.002) or ARBs (OR=0.17; 95% CI, 0.05%-0.54%; P=0.003), compared to other patients. The odds of having an untreated indication were significantly higher among patients with a history of heart failure (OR=5.7; 95% CI, 3.43%-7.41%; P=0.005), while these odds were 98% lower among those using lipid-lowering agents (OR=0.02; 95% CI, 0.01%-0.24%; P<0.001), compared to other patients.
Discussion
This study investigated the DRPs among T2D patients with hypertension in Lebanon, and assessed the predictors of these problems. The DRPs were mostly related to treatment effectiveness, including the non-optimal effect of drugs and existence of an untreated indication. The most common causes of DRPs were related to drug selection and dose selection. The predictors of non-optimal drug treatment effect were the elevated creatinine level, lipid-lowering drug use, ACEI use, ARB use, and anti-anginal agent use. The odds of untreated indication varied among those with a history of heart failure or those using lipid-lowering agents. The number of DRPs among T2D patients in the present study was significantly lower compared to the results of other similar studies [16, 26]. A recent meta-analysis found more DRPs in T2D patients with hypertension than in those with T2D alone [27]. Although DRPs are common among patients with T2D [28], the difference in the sampling methods and the authors’ knowledge can affect their identification and evaluation. Most patients in our study had at least one DRP, similar to other studies [16, 29], but their number was much higher than that reported a hospital-based study in India [30]. This finding can be explained by the presence of underlying diseases, which leads to the use of several treatment options and, as a result, a higher risk of errors. Other studies reported lower percentages of problems related to non-optimal effect of drugs [12, 16], possibly due to the comparison with international treatment guidelines which may not be applied in Lebanese hospitals. The untreated indication problem in our study was significantly higher than in the studies by Rochon et al. and Zaman et al. [12, 16]. This can be related to the unavailability of some drugs in the hospitals [31, 32], leading to their non-prescription despite the needs of patients. Drug selection was the primary cause of DRPs, in agreement with the PCNE classification that links the treatment effectiveness-related problem to drug selection or dose selection [23]. In our study, the number of identified causes was lower than in previous studies [16, 33], possibly due to the adaptation of the problems to the most applicable cause and not to multiple reasons. Comorbidities in T2D patients necessitate the use of polypharmacy [34], which was found to be associated with DRPs [35, 36]. This association was not significant in our study, possibly due to the effect of polypharmacy.
The odds of non-optimal drug treatment were higher among patients with elevated creatinine levels. Renal problems require a dose adjustment and routine monitoring [7] which may cause DRPs. T2D is also a predictor of DRPs [37], and can increase the risk. The odds of non-optimal drug treatment were also higher among those using lipid-lowering or anti-anginal agents, consistent with the findings of a recent study in France [38]. However, the odds were significantly lower among those who achieved the HbA1C target level than other patients. Lower HbA1C level is associated with better metabolic control [39] and, thus, a lower risk of complications and drug use. The odds of untreated indication were significantly higher among patients with a history of heart failure. This can be explained by the cardiac remodeling caused by heart failure resulting in cardiac dysfunction [40] and, as a result, other complications are left untreated [41]. Findings from the present study highlight the importance of hospital pharmacists in assessing DRPs, given that pharmacist-led medication reconciliation was found to be associated with potentially inappropriate medication deprescribing and decreased hospital re-admissions [42]. The clinical integration of a pharmacist in the medical team can improve pharmaceutical and medical care and ensure the production of a reliable medication history [43].
This study had some limitations and strengths. Due to the use of a self-report tool for data collection, there might be recall bias. However, information was validated according to the medical records. The bias was reduced since the pharmacists were uniformly trained and did not interfere with the patient’s answers. Moreover, data coding and analysis were performed by a different researcher, which minimized the subjectivity in data collection. A longitudinal study with larger sample size is recommended in Lebanon and other countries.
Conclusion
There is a high prevalence of DRPs in hospitalized T2D patients with hypertension in Lebanon. The predictors of such problems should be taken into consideration for the management of these patients. Findings of this study emphasize the need for integrating a clinical pharmacist in general practice to detect inappropriate prescriptions and prevent adverse drug events.
Ethical Considerations
Compliance with ethical guidelines
The protocol of this study was approved by the Institutional Review Board of the Faculty of Pharmacy at the Lebanese University and the Hospital’s Ethical Committee (Code: 20/21/C; February 19th, 2021). Data were kept confidential. Written informed consent was obtained from the patient. They were free to leave the study at any time.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, formal analysis and validation: Georges Hatem; Project administration: Dalia Khachman; Methodology: Aya Awarkeh, Lynne H Jaffal, Dalia Khachman and Amal Al-Hajje; Data curation: Aya Awarkeh, Lynne H Jaffal and Salam Zein; Review and editing: Georges Hatem, Salam Zein, Dalia Khachman and Amal Al-Hajje; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Nathalie Lahoud for her assistance in data analysis.
References
The prevalence of type 2 diabetes (T2D) have significantly increased, having upward trend [1] and high clinical and public health burden [2]. There are several modifiable risk factors for T2D. Adequate management of these risk factors can reduce mortality and the occurrence of comorbidities [3]. T2D is associated with an increased risk of cardiovascular diseases (CVD) such as myocardial infarction, ischemic stroke, heart failure, and aortic valve stenosis [4]. Drug-related problems are common among T2D patients and can negatively affect their quality of life [5]. The T2D patients with hypertension are at a higher risk of drug-related problems (DRPs), considering the number of medications used for their treatment [6]. These problems can induce mortality and morbidity among patients and extend their hospitalization due to the challenges in controlling their blood pressure and the diabetes-related complications [7].
The DRPs can be prevented [8] and lead to significantly lower health expenditures [9]. Several factors can increase the risk of DRPs in T2D patients with hypertension. The main reported factors are polypharmacy, older age, and underlying diseases [10]. A recent cross-sectional study found that, for every one unit increase in the number of medications, the odds of DRPs increased by 10% [11]. Inappropriate prescribing, over-the-counter drug use, and low adherence to treatment can also increase the risk of DRPs [12]. Older patients are more prone to DRPs and require interventions to manage some problems, such as the use of expired medications and drug storage issues [13]. Inpatients and those with many chronic conditions are also at a higher risk of developing DRPs [14].
A recent study investigated DRPs among T2D patients in Lebanon [15]. However, no study was found on hospitalized T2D patients with hypertension in Lebanon. There are few studies investigated them in other countries. Understanding DRPs can help make informed health decisions and effectively manage these patients. Therefore, this study aims to investigate DRPs and their causes among T2D patients with hypertension and to find the predictors of these problems.
Materials and Methods
Study design and samples
This is an observational cross-sectional study that was conducted for six months (March-September 2021) on patients diagnosed with T2D and hypertension admitted to the internal medicine department of a tertiary care hospital in Lebanon. Adult patients receiving one or more anti-diabetes drugs and at least one medication for CVD or hypertension were included. The criteria based on sex, age, and ethnicity were not used. The sample size was determined using the Epi Info software, version 7. Based on findings from a previous study [16], 90.5% of T2D patients had at least one DRP. Considering a 95% confidence interval and a 5% margin of error, the minimum sample size was 133.
Data collection
After explaining the study objectives orally to the patients for 15 minutes and inviting them to participate in the study, their written informed consent was obtained. For surveying their characteristics, a questionnaire was developed in English based on the literature review [14, 17]. It was tested in a pilot study on 10 patients, and the items that needed more clarity were either modified or deleted. The adequacy of the instrument was examined based on a technique recommended in a previous study [18]. Positive inter-item correlations [ranging 0.25-0.35), test re-test reliability of 0.807, and a Cronbach α of 0.737 were obtained, indicating the adequacy of the designed questionnaire. The first part surveys the general characteristics of participants such as sex, age (<65 or ≥65), height, weight, educational level (illiterate, primary school, secondary school, academic), employment status, marital status, medical insurance coherence, and lifestyle habits such as smoking, alcohol and coffee consumption, physical activity and its frequency, and the recommended type of diet (low-carbohydrates, low-salt, or low-fat). The second part surveys the medical and medication history: Duration of diabetes and CVD, glycosylated hemoglobin A1C (HbA1C) level (target level <7%) [19], other associated diseases, name, dosage, and administration of used medications, and the reason for hospitalization.
Based on the information obtained by the instruments as well as those extracted from the patients’ medical records, effectiveness of diabetes and CVD treatment, drug indication, drug contraindication, drug dosage, drug combinations, and adverse drug reactions (ADR) were evaluated [20-22]. The Pharmaceutical Care Network Europe (PCNE) classification system, version 7 was used to categorize the DRPs [23]. Three domains of problems (treatment effectiveness, adverse safety, and other) and three domains of causes (drug selection, dose selection, and other) based on the PCNE classification were assessed.
Statistical analysis
Statistical analyses were performed in SPSS software, version 27 (SPSS Inc, Chicago, Illinois). Based on the values of the skewness (0.027) and kurtosis (0.470), the data were found to have normal distribution and met the expected values [24]. The body mass index (BMI) of patients was calculated by dividing the weight (in kilograms) by the height (in meters squared). Then, the patients were categorized based on BMI according to the recommended criteria [25]. Categorical variables were presented by frequency and percentage. The data related to age, duration of diabetes and other comorbidities, and number of drugs per patient were described by Mean±SD. Bivariate analysis was conducted on the dichotomous dependent variable (DRPs). Independent-sample t-test was performed over continuous independent variables, and chi-square/Fisher’s exact test were used for categorical variables. Binary logistic regression was done on the two most frequent DRPs producing odd ratios (ORs) at a 95% confidence interval (CI). The Risk factors with P<0.20 were in bivariate analyses. A P<0.05 was considered statistically significant. The statistical model for finding the predictors of non-optimal treatment effect had a P<0.001 in Omnibus test, (Nagelkerke R square=0.411). The model for finding the predictors of an untreated indication also had a P<0.001 in Omnibus test (Nagelkerke R square=0.919).
Results
General characteristics of the patients
Overall, 146 eligible patients participated, out of whom 135(92.5%) completed the survey. Table 1 represents their general characteristics and lifestyle. Most of them were female (57% vs. 43% male). Their mean age was 70.2±11.1 years; 100(74.1%) <65 years, and 35 (25.9%) ≥65 years. About 25% of patients had a normal BMI; most of them were overweight (31.9%) or obese (40%). Most patients were married (60.7%) and illiterate (47.4%) or with a primary school education (35.6%). Almost 80% were unemployed, and 92.6% had a family caregiver. Regards lifestyle factors, only 23.7% were smokers; 20.7% had physical activity for less than 150 minutes per week, and 67.4% were coffee consumers. Low-carbohydrate, low-salt, or low-fat diets were adopted by about one-third of patients
Medical and medication history
Table 2 shows the statistics for medical and medication history of the patients. Most of patients (64.4%) had been hospitalized for seven days or less. Hospitalization rate related to diabetes and CVD was 17.0% and 26.7%, respectively. The mean duration of diabetes was 12.5±7.8 years, and only 38.6% achieved the target level of HbA1C. Retinopathy was the most common associated complication (57.0%), followed by diabetic foot (17.0%). The mean duration of hypertension was 10.0±7.0 years. The CVDs were coronary artery disease (62.2%), heart failure (13.3%), and stroke (11.9%). Other comorbidities were renal insufficiency (77.0%) and dyslipidemia (20.0%). Sixty percentage of patients were treated by insulin alone in the hospital, and the rest (40%) by combination of insulin and oral antidiabetics including dipeptidyl peptidase-4 (DPP4) inhibitors (24.4%) and metformin (23.7%). The most common antihypertensive and CVD drugs were beta blockers (69.6%), antiplatelet agents (63.7%), lipid-lowering drugs (57.8%), and diuretics (49.6%).
Drug-related problems and causes
The identified DRPs and their causes are presented in Table 3. The most reported problems were related to treatment effectiveness (88.1%). Most of these problems were related to the non-optimal effect of drug treatment (48.2%), and untreated indication (38.3%). The causes of these problems were primarily related to drug selection or dose selection (72.0% and 21.8%, respectively). One of the reported causes was the lack of receiving a synergistic medication (46.0%). In this study, 31 patients did not receive angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB), despite having a history of atherosclerotic CVD or microalbuminuria. The absence of primary or secondary prevention of CVD without contraindication was also reported in patients with lower limb edema. Moreover, 12 patients received moderate-intensity statin instead of high-intensity statin. Other patients received inadequate medications (enoxaparin, saxagliptin, trandolapril, and moxonidine). The most prescribed drugs in the presence of contraindication were six moxonidine cases with a creatinine clearance (ClCr) <30 mL/min, two metformin cases (ClCr <30 mL/min), and three trimetazidine cases (ClCr <30 mL/min, Parkinson disease). Other problems were also reported such as hypotension (due to the combination of several antihypertensive drugs), hyperkalemia, hyponatremia (due to the combination of diuretics), and hypoglycemia (due to insulin). Serum creatinine level was significantly higher in patients who had DRPs (1.35 vs. 0.94 mg/dL; P=0.004) and those with the problem “non-optimal effect of drug treatment” (1.44 vs. 1.07 mg/dL; P=0.006).
Predictors of DRPs
Table 4 presents the predictors of non-optimal treatment effect and the existence of an untreated indication. After adjusting the effect of covariates, the odds of non-optimal drug treatment effect were 2.32 times higher for patients with elevated serum creatinine level compared to those with normal values (OR=2.32; 95% CI, 1.04%-5.21%; P=0.042). These odds were also higher if patients used lipid-lowering agents (OR=3.67; 95% CI, 1.36%-9.89%; P=0.010) or anti-anginal agents (OR=3.71; 95% CI, 1.18%-11.71%; P=0.025), compared to non-users. Moreover, the odds of non-optimal treatment effect were 67% lower among patients with an achieved HbA1C target level compared to those with abnormal levels (OR=0.33; 95% CI, 0.15%-0.76%; P=0.009). They were also lower among patients using ACEIs (OR=0.14; 95% CI: 0.04-0.47; P=0.002) or ARBs (OR=0.17; 95% CI, 0.05%-0.54%; P=0.003), compared to other patients. The odds of having an untreated indication were significantly higher among patients with a history of heart failure (OR=5.7; 95% CI, 3.43%-7.41%; P=0.005), while these odds were 98% lower among those using lipid-lowering agents (OR=0.02; 95% CI, 0.01%-0.24%; P<0.001), compared to other patients.
Discussion
This study investigated the DRPs among T2D patients with hypertension in Lebanon, and assessed the predictors of these problems. The DRPs were mostly related to treatment effectiveness, including the non-optimal effect of drugs and existence of an untreated indication. The most common causes of DRPs were related to drug selection and dose selection. The predictors of non-optimal drug treatment effect were the elevated creatinine level, lipid-lowering drug use, ACEI use, ARB use, and anti-anginal agent use. The odds of untreated indication varied among those with a history of heart failure or those using lipid-lowering agents. The number of DRPs among T2D patients in the present study was significantly lower compared to the results of other similar studies [16, 26]. A recent meta-analysis found more DRPs in T2D patients with hypertension than in those with T2D alone [27]. Although DRPs are common among patients with T2D [28], the difference in the sampling methods and the authors’ knowledge can affect their identification and evaluation. Most patients in our study had at least one DRP, similar to other studies [16, 29], but their number was much higher than that reported a hospital-based study in India [30]. This finding can be explained by the presence of underlying diseases, which leads to the use of several treatment options and, as a result, a higher risk of errors. Other studies reported lower percentages of problems related to non-optimal effect of drugs [12, 16], possibly due to the comparison with international treatment guidelines which may not be applied in Lebanese hospitals. The untreated indication problem in our study was significantly higher than in the studies by Rochon et al. and Zaman et al. [12, 16]. This can be related to the unavailability of some drugs in the hospitals [31, 32], leading to their non-prescription despite the needs of patients. Drug selection was the primary cause of DRPs, in agreement with the PCNE classification that links the treatment effectiveness-related problem to drug selection or dose selection [23]. In our study, the number of identified causes was lower than in previous studies [16, 33], possibly due to the adaptation of the problems to the most applicable cause and not to multiple reasons. Comorbidities in T2D patients necessitate the use of polypharmacy [34], which was found to be associated with DRPs [35, 36]. This association was not significant in our study, possibly due to the effect of polypharmacy.
The odds of non-optimal drug treatment were higher among patients with elevated creatinine levels. Renal problems require a dose adjustment and routine monitoring [7] which may cause DRPs. T2D is also a predictor of DRPs [37], and can increase the risk. The odds of non-optimal drug treatment were also higher among those using lipid-lowering or anti-anginal agents, consistent with the findings of a recent study in France [38]. However, the odds were significantly lower among those who achieved the HbA1C target level than other patients. Lower HbA1C level is associated with better metabolic control [39] and, thus, a lower risk of complications and drug use. The odds of untreated indication were significantly higher among patients with a history of heart failure. This can be explained by the cardiac remodeling caused by heart failure resulting in cardiac dysfunction [40] and, as a result, other complications are left untreated [41]. Findings from the present study highlight the importance of hospital pharmacists in assessing DRPs, given that pharmacist-led medication reconciliation was found to be associated with potentially inappropriate medication deprescribing and decreased hospital re-admissions [42]. The clinical integration of a pharmacist in the medical team can improve pharmaceutical and medical care and ensure the production of a reliable medication history [43].
This study had some limitations and strengths. Due to the use of a self-report tool for data collection, there might be recall bias. However, information was validated according to the medical records. The bias was reduced since the pharmacists were uniformly trained and did not interfere with the patient’s answers. Moreover, data coding and analysis were performed by a different researcher, which minimized the subjectivity in data collection. A longitudinal study with larger sample size is recommended in Lebanon and other countries.
Conclusion
There is a high prevalence of DRPs in hospitalized T2D patients with hypertension in Lebanon. The predictors of such problems should be taken into consideration for the management of these patients. Findings of this study emphasize the need for integrating a clinical pharmacist in general practice to detect inappropriate prescriptions and prevent adverse drug events.
Ethical Considerations
Compliance with ethical guidelines
The protocol of this study was approved by the Institutional Review Board of the Faculty of Pharmacy at the Lebanese University and the Hospital’s Ethical Committee (Code: 20/21/C; February 19th, 2021). Data were kept confidential. Written informed consent was obtained from the patient. They were free to leave the study at any time.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, formal analysis and validation: Georges Hatem; Project administration: Dalia Khachman; Methodology: Aya Awarkeh, Lynne H Jaffal, Dalia Khachman and Amal Al-Hajje; Data curation: Aya Awarkeh, Lynne H Jaffal and Salam Zein; Review and editing: Georges Hatem, Salam Zein, Dalia Khachman and Amal Al-Hajje; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Nathalie Lahoud for her assistance in data analysis.
References
- Magliano DJ, Islam RM, Barr ELM, Gregg EW, Pavkov ME, Harding JL, et al. Trends in incidence of total or type 2 diabetes: Systematic review. BMJ. 2019; 366:l5003. [DOI:10.1136/bmj.l5003] [PMID] [PMCID]
- Forouhi NG, Wareham NJ. Epidemiology of diabetes. Medicine. 2019; 47(1):22-7. [DOI:10.1016/j.mpmed.2018.10.004]
- Rawshani A, Rawshani A, Franzén S, Sattar N, Eliasson B, Svensson AM, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2018; 379(7):633-44. [DOI:10.1056/NEJMoa1800256] [PMID]
- Larsson SC, Wallin A, Håkansson N, Stackelberg O, Bäck M, Wolk A. Type 1 and type 2 diabetes mellitus and incidence of seven cardiovascular diseases. Int J Cardiol. 2018; 262:66-70. [DOI:10.1016/j.ijcard.2018.03.099] [PMID]
- Wagner ML, McCarthy C, Bateman MT, Simmons D, Prioli KM. Pharmacists improve diabetes outcomes: A randomized controlled trial. J Am Pharm Assoc (2003). 2022; 62(3):775-82.e3. [DOI:10.1016/j.japh.2021.12.015] [PMID]
- Yan L, Ji N, Xu J, Liu M, Guan L, Liu K, et al. Evaluating behavioral risk factor interventions for hypertensive and diabetic patient management in the national basic public health service programs from 2009. China CDC Weekly. 2022; 4(19):411-6. [PMID] [PMCID]
- Garin N, Sole N, Lucas B, Matas L, Moras D, Rodrigo-Troyano A, et al. Drug related problems in clinical practice: A cross-sectional study on their prevalence, risk factors and associated pharmaceutical interventions. Sci Rep. 2021; 11(1):883. [DOI:10.1038/s41598-020-80560-2] [PMID] [PMCID]
- Blum MR, Sallevelt BTGM, Spinewine A, O'Mahony D, Moutzouri E, Feller M, et al. Optimizing Therapy to Prevent Avoidable Hospital Admissions in Multimorbid Older Adults (OPERAM): Cluster randomised controlled trial. BMJ. 2021; 374:n1585. [DOI:10.1136/bmj.n1585] [PMID] [PMCID]
- Ruiz-Ramos J, Juanes-Borrego A, Puig-Campany M, Blazquez-Andión M, López-Vinardell L, Gilabert-Perramon A, et al. Cost-effectiveness analysis of implementing a secondary prevention programme in those patients who visited an emergency department for drug-related problems. Int J Pharm Pract. 2022; 30(5):434-40. [DOI:10.1093/ijpp/riac061] [PMID]
- El Morabet N, Uitvlugt EB, van den Bemt BJF, van den Bemt PMLA, Janssen MJA, Karapinar-Çarkit F. Prevalence and preventability of drug-related hospital readmissions: A systematic review. J Am Geriatr Soc. 2018; 66(3):602-8. [DOI:10.1111/jgs.15244] [PMID]
- Almodóvar AS, Nahata MC. Associations between chronic disease, polypharmacy, and medication-related problems among medicare beneficiaries. J Manag Care Spec Pharm. 2019; 25(5):573-7. [DOI:10.18553/jmcp.2019.25.5.573] [PMID] [PMCID]
- Rochon PA, Petrovic M, Cherubini A, Onder G, O'Mahony D, Sternberg SA, et al. Polypharmacy, inappropriate prescribing, and deprescribing in older people: Through a sex and gender lens. Lancet Healthy Longev. 2021; 2(5):e290-300. [DOI:10.1016/S2666-7568(21)00054-4] [PMID]
- Beuscart JB, Petit S, Gautier S, Wierre P, Balcaen T, Lefebvre JM, et al. Polypharmacy in older patients: Identifying the need for support by a community pharmacist. BMC Geriatr. 2019; 19(1):277. [DOI:10.1186/s12877-019-1276-y] [PMID] [PMCID]
- Hailu BY, Berhe DF, Gudina EK, Gidey K, Getachew M. Drug related problems in admitted geriatric patients: The impact of clinical pharmacist interventions. BMC Geriatr. 2020; 20(1):13. [DOI:10.1186/s12877-020-1413-7] [PMID] [PMCID]
- Amena A, Amal AH, Salam Z, Sanaa A, Samar R. Evaluation of drug related problems in patients with type 2 diabetes. J Diabetes Res Rev Rep. SRC/JDRR-166. 2022; 4(3):1-11. [DOI:doi.org/10.47363/JDRR/2022(4)159]
- Zaman Huri H, Fun Wee H. Drug related problems in type 2 diabetes patients with hypertension: A cross-sectional retrospective study. BMC Endocr Disord. 2013; 13:2.[DOI:10.1186/1472-6823-13-2] [PMID] [PMCID]
- Verdoorn S, Kwint HF, Blom JW, Gussekloo J, Bouvy ML. Effects of a clinical medication review focused on personal goals, quality of life, and health problems in older persons with polypharmacy: A randomised controlled trial (DREAMeR-study). PLOS Med. 2019; 16(5):e1002798. [DOI:10.1371/journal.pmed.1002798] [PMID] [PMCID]
- Hertzog MA. Considerations in determining sample size for pilot studies. Res Nurs Health. 2008; 31(2):180-91. [DOI:10.1002/nur.20247] [PMID]
- Elgart JF, Silvestrini C, Prestes M, Gonzalez L, Rucci E, Gagliardino JJ. Drug treatment of type 2 diabetes: Its cost is significantly associated with HbA1c levels. Int J Clin Pract. 2019; 73(4):e13336. [DOI:10.1111/ijcp.13336] [PMID]
- Bakris G, Ali W, Parati G. ACC/AHA versus ESC/ESH on hypertension guidelines: JACC guideline comparison. J Am Coll Cardiol. 2019; 73(23):3018-26. [DOI:10.1016/j.jacc.2019.03.507] [PMID]
- Guerrero-García C, Rubio-Guerra AF. Combination therapy in the treatment of hypertension. Drugs Context. 2018; 7:212531. [DOI:10.7573/dic.212531] [PMID] [PMCID]
- LeRoith D, Biessels GJ, Braithwaite SS, Casanueva FF, Draznin B, Halter JB, et al. Treatment of diabetes in older adults: An endocrine society* clinical practice guideline. J Clin Endocrinol Metab. 2019; 104(5):1520-74. [DOI:10.1210/jc.2019-00198] [PMID] [PMCID]
- Özdemir N, Kara E, Büyükçam A, Aykaç K, Çeliker A, Demirkan K, et al. Evaluation of medication errors in pediatric patients using antibiotics. Turk J Pediatr. 2021; 63(6):970-7. [DOI:10.24953/turkjped.2021.06.004] [PMID]
- Hatem G, Zeidan J, Goossens M, Moreira C. Normality testing methods and the importance of skewness and kurtosis in statistical analysis. BAU J Sci Tech. 2022; 3(2):1-5. [DOI:10.54729/KTPE9512]
- Weir CB, Jan A. BMI classification percentile and cut off points. 2023; In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. [PMID]
- Yimama M, Jarso H, Desse TA. Determinants of drug-related problems among ambulatory type 2 diabetes patients with hypertension comorbidity in Southwest Ethiopia: A prospective cross sectional study. BMC Res Notes. 2018; 11(1):679. [DOI:10.1186/s13104-018-3785-8] [PMID] [PMCID]
- Enumula D, Rashid M, Sharma S, GirishThunga SK, Acharya LD. Drug related problems in type-2-diabetes mellitus with and without cardiovascular diseases: A systematic review and meta-analysis. Ann Romn Soc Cell Biol. 2021; 25(4):12623-42. [Link]
- Sheleme T, Sahilu T, Feyissa D. Identification and resolution of drug-related problems among diabetic patients attending a referral hospital: A prospective observational study. J Pharm Policy Pract. 2021; 14(1):50. [DOI:10.1186/s40545-021-00332-9] [PMID] [PMCID]
- Alomi YA, Al-Shaibani AS, Alfaisal G, Alasmi NM. Cost analysis of drug-related problems in Saudi Arabia: Patients’ and healthcare providers’ perspective. J Pharm Pract Community Med. 2018; 4(2):107-12. [DOI:10.5530/jppcm.2018.2.24]
- Prasad TSD, Ranganayakulu D, Devanna N. Prescribing pattern and medication related problems in hospitalized diabetic patients: A hospital-based study. J Pharm Res Int. 2021; 33(5):12-21. [DOI:10.9734/jpri/2021/v33i531177].
- Al-Aqeel SA, Al-Salloum HF, Abanmy NO, Al-Shamrani ASA. Undispensed prescriptions due to drug unavailability at a teaching hospital in Saudi Arabia. Int J Health Res. 2010; 3(4):213-6. [DOI:10.4314/ijhr.v3i4.70424]
- Hatem G, Goossens M. Health care system in Lebanon: A review addressing health inequalities and ethical dilemmas of frontline workers during COVID-19 pandemic. BAU J Health Wellbeing. 2022; 5(1):1-11. [DOI:10.54729/YVAA4887]
- Chan DC, Chen JH, Kuo HK, We CJ, Lu IS, Chiu LS, et al. Drug-related problems (DRPs) identified from geriatric medication safety review clinics. Arch Gerontol Geriatr. 2012; 54(1):168-74. [DOI:10.1016/j.archger.2011.02.005] [PMID]
- Ballaziri H, Aziz SE, Chadli A. The diabetes mellitus type 2 in elderly patients: Comorbidities and polymedication (about 300 cases). 2019; 63:925. [DOI:10.1530/endoabs.63.P925]
- Tang J, Wang K, Yang K, Jiang D, Fang X, Su S, et al. A combination of Beers and STOPP criteria better detects potentially inappropriate medications use among older hospitalized patients with chronic diseases and polypharmacy: A multicenter cross-sectional study. BMC Geriatr. 2023; 23(1):44. [DOI:10.1186/s12877-023-03743-2] [PMID] [PMCID]
- Montero-Suárez M, Souto-Pereira M, Vazquez-Lago JM, Portela-Romero M. Analysis of drug-related problems in polymedicated patients over the age of 64 in primary care. A cross-sectional descriptive study. Enferm Clin (Engl Ed). 2021; 31(1):36-44. [DOI:10.1016/j.enfcle.2019.12.007] [PMID]
- Mechessa DF, Kebede B. Drug-related problems and their predictors among patients with diabetes attending the Ambulatory Clinic of Gebre Tsadik Shawo General Hospital, Southwest Ethiopia. Diabetes Metab Syndr Obes. 2020; 13:3349-57. [DOI:10.2147/DMSO.S267790] [PMID] [PMCID]
- Cerfon MA, Vernaudon J, Gervais F, Morelon E, Coste MH, Krolak-Salmon P, et al. Drug-related problems in older patients with advanced chronic kidney disease identified during pretransplant comprehensive geriatric assessment. Nephrol Ther. 2022; 18(1):45-51.[DOI:10.1016/j.nephro.2021.08.006] [PMID]
- Van Loocke M, Battelino T, Tittel SR, Prahalad P, Goksen D, Davis E, Casteels K; SWEET study group. Lower HbA1c targets are associated with better metabolic control. Eur J Pediatr. 2021; 180(5):1513-20. [DOI:10.1007/s00431-020-03891-2] [PMID]
- Bell DSH, Goncalves E. Heart failure in the patient with diabetes: Epidemiology, aetiology, prognosis, therapy and the effect of glucose-lowering medications. Diabetes Obes Metab. 2019; 21(6):1277-90. [DOI:10.1111/dom.13652] [PMID]
- Ferrini M, Johansson I, Aboyans V. Heart failure and its complications in patients with diabetes: Mounting evidence for a growing burden. Eur J Prev Cardiol. 2019; 26(2_suppl):106-13. [DOI:10.1177/2047487319885461] [PMID]
- Jovevski JJ, Smith CR, Roberts JL, Dev S, Iloabuchi TC, Gruber EA, et al. Implementation of a compulsory clinical pharmacist-led medication deprescribing intervention in high-risk seniors in the emergency department. Acad Emerg Med. 2023; 30(4):410-9. [DOI:10.1111/acem.14699] [PMID]
- Goulas C, Lohan L, Laureau M, Perier D, Pinzani V, Faucanie M, et al. Involvement of pharmacists in the emergency department to correct errors in the medication history and the impact on adverse drug event detection. J Clin Med. 2023; 12(1):376. [DOI:10.3390/jcm12010376] [PMID] [PMCID]
Type of Study: Original Research |
Subject:
Clinical Pharmacy
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
